
Cataract surgery in patients with underlying diabetes is not limited to simply replacing a clouded lens. It is a delicate process that must also evaluate the condition of the retina deep inside the eye. Rather than stopping at checking blood sugar levels alone, a comprehensive and detailed retinal assessment is essential to reasonably expect a safe recovery of vision.
“If I have diabetes, is eye surgery much more complicated and risky?”

This is a question many patients with diabetes ask when they come to the clinic. Quite a few people delay surgery out of concern about diabetic complications and end up leaving worsening vision unaddressed. In real clinical practice, however, there are clear criteria used to judge surgical safety and determine timing. Knowing these criteria can reduce vague anxiety and help you prepare in a practical way.
When determining whether cataract surgery is feasible for a patient with diabetes, the first thing clinicians look at is not the blood sugar number itself. Beyond the visible cataract, the evaluation of whether the retina—the innermost part of the eye—can tolerate the surgical process often determines the overall direction of treatment.
1. If you have diabetes, what is the “real variable” that makes cataract surgery riskier?
Having diabetes alone does not automatically make cataract surgery contraindicated or impossible. In fact, many people with diabetes experience meaningful improvement in vision after surgery. What truly influences outcomes is whether retinal complications—such as diabetic retinopathy or diabetic macular edema—are present.
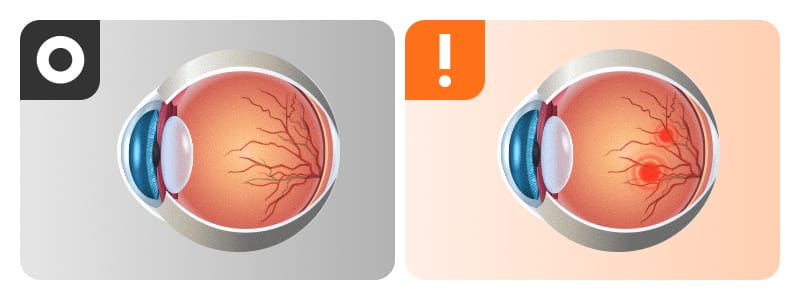
When vision becomes blurry, it is easy to suspect cataracts first. However, in patients with diabetes, decreased vision may not be caused only by lens clouding. Over time, diabetes can damage the tiny blood vessels inside the eye and can also cause swelling in the macula, which is responsible for central vision.
You can think of the eye like a camera. A cataract is like a cloudy “lens” at the front of the camera. Diabetic retinopathy, on the other hand, is like damage to the “film (image sensor)” at the back. Even if you replace the lens with a clear new one, you cannot get a sharp photo if the film is already damaged. This is why both the “lens” and the “film” must be evaluated before cataract surgery.
2. Key pre-op tests for diabetic cataract surgery: dilated fundus exam and OCT
Preoperative evaluation for patients with diabetes is not simply about confirming “whether surgery is possible.” It is more like creating a blueprint for “in what order, and how, follow-up will be done going forward.” The core tool for drawing this blueprint is the dilated fundus exam. By dilating the pupil and directly examining the entire retina, clinicians can determine whether diabetic retinopathy is present—an essential starting point.
Diabetic retinopathy is broadly classified into non-proliferative and proliferative types, and non-proliferative disease is further divided into three stages depending on severity. Proliferative disease refers to the development of abnormal “new blood vessels” in the retina. This can lead to retinal and vitreous hemorrhage or membrane formation, potentially causing severe vision loss that may be difficult to recover from even with later surgery. Therefore, a key treatment goal is to suppress progression—before it reaches the proliferative stage—through measures such as retinal laser treatment or intraocular injections.
After the dilated fundus exam, an OCT (optical coherence tomography) scan—which captures cross-sectional images of the retina—may also be needed. OCT can precisely identify subtle structural abnormalities and determine whether macular edema, which can be critical to vision, is present. Early retinal complications often progress quietly without noticeable symptoms. In fact, according to domestic reports, the rate of fundus examination within the past year among Korean patients with diabetes aged 40 and older is only about 29.5%. For this reason, even without symptoms, a detailed preoperative exam is necessary to accurately diagnose the condition of the “film” deep in the eye and to make a reasonable
prediction of postoperative outcomes.
Ultimately, the dilated fundus exam and OCT are the process of checking the film before changing the lens—and they should not be separated.
✅ Pre-op essential checklist
- Have you confirmed the presence or absence of diabetic retinopathy with a dilated fundus exam within the past year?
- Have you been told whether the cause of decreased vision is cataract alone, or whether retinal complications are also present?
- If needed, has an OCT plan been established to check for macular edema?
3. Is lowering HbA1c enough? What a “single number” can miss
HbA1c reflects average blood glucose over the past 2–3 months and plays an important role in assessing overall systemic condition before surgery. However, it is difficult to conclude surgical risk based only on “a single HbA1c value.” Large clinical studies have also reported evidence that postoperative complication risk is not determined immediately by one specific number alone.
That does not mean blood sugar control is unimportant. Blood sugar management is like stabilizing the workbench for a precise operation. In patients with diabetes whose glucose is not well controlled, the likelihood of corneal endothelial swelling after cataract surgery is higher than in people without diabetes. While it often improves with medication, this is a representative reason why preoperative glucose control matters.
Therefore, when deciding surgical timing, clinicians evaluate the following three elements together rather than relying on a single number.
| Assessment Items | Purpose of Evaluation | Impact on Surgical Planning |
|---|---|---|
| Systemic Condition (Blood sugar fluctuations, comorbidities) |
Assessing perioperative infection risk and recovery capacity | Determining the need for interdepartmental consultation and scheduling optimal surgery timing |
| Fundus Condition (Presence of retinal/macular edema) |
Identifying underlying causes of vision loss | Deciding whether prior retinal treatment is required and setting expected visual outcomes |
| Feasibility of Long-Term Follow-Up |
Early detection of and response to post-operative changes | Establishing follow-up intervals and planning long-term retinal monitoring |
Trying to force blood sugar down rapidly right before surgery can, depending on a person’s overall condition, become an added burden. Rather than giving up on surgery or pushing too hard because of a number, it is preferable to set a safe surgical timing through close coordinated care between internal medicine and ophthalmology.
4. Why multifocal lens selection requires extra caution in patients with diabetes

Once you decide to proceed with cataract surgery, you will choose the type of intraocular lens, such as monofocal or multifocal. Recently, interest in multifocal lenses—which can reduce dependence on reading glasses—has been very high. However, if you have diabetes, lens selection must be approached much more carefully than in typical situations, and the prerequisite should be only one thing: retinal status.
Multifocal lenses use an optical design that splits incoming light into multiple focal points. Because the light is divided, the retina (the “film”), which is neural tissue, must be very healthy to fully benefit. If you have a history of treatment for diabetic retinopathy or even subtle macular swelling, the macular retina affected by diabetic edema may not properly process the dispersed light from a multifocal lens, and postoperative vision may fall short of expectations.
Therefore, before asking “Which lens is more convenient?” you should first confirm, “Is my retina currently able to receive light properly?” If the fundus findings are very stable, a wider range of choices may be possible. But if retinal complications are observed, a monofocal lens—which concentrates light into a single focus—may be a more straightforward and safer choice in terms of visual quality.
5. Why the “first year” after cataract surgery matters: the retina can change quietly
For patients with diabetes, cataract surgery is not a short event that ends the moment you walk out of the operating room. From a medical perspective, true completion of treatment is achieved only after at least one year of postoperative follow-up.
When related studies are considered together, the subtle inflammatory response that occurs during surgery may affect retinal blood vessels deep in the eye. As a result, there are reports that existing diabetic retinopathy may progress or that macular edema may newly appear within one year after surgery. The impact of replacing the lens can re-stimulate a film that had been relatively quiet.
Even if you are satisfied with clearer vision right after surgery, if several months later your central vision looks distorted or becomes blurry again, it may be a sign of retinal change. Therefore, if you anticipate having to stop follow-up care soon after surgery due to living abroad or a busy schedule, it is safer to re-discuss the timing of surgery itself with your medical team. Postoperative care is not merely passive defense against side effects—it is an active part of treatment to protect functional vision.
✅ Post-op 1-year follow-up checklist
- Is there a long-term retinal follow-up schedule (fundus exam/OCT) at 1 month, 3 months, and 1 year after surgery?
- If symptoms such as visual distortion or central blurring occur, can you respond immediately?
- Are you coordinating stable blood sugar management goals with internal medicine in line with your ophthalmology follow-up schedule?
6. Frequently Asked Questions (FAQ)
Q. If my HbA1c is high, should I postpone cataract surgery right away?
Surgical feasibility is not determined by the HbA1c number alone. While glucose indicators are important, the priority is to carefully adjust timing under coordinated care with internal medicine by comprehensively evaluating systemic stability, fundus status (retina/macula), and the postoperative follow-up plan.
Q. Why do I need a fundus exam and OCT before surgery?
In patients with underlying diabetes, retinal complications that reduce vision can accompany lens clouding (cataract) without symptoms. If the exam shows a wide range of dot hemorrhages in the retina or macular edema, appropriate treatment—such as retinal laser and intraocular injections—is needed to prevent diabetic retinopathy from worsening further. A preoperative fundus exam and, when needed, OCT are essential for creating the blueprint to determine the order of treatment and to choose the lens.
Q. Can my vision become blurry again after cataract surgery?
Subtle inflammation or stimulation during surgery can affect deeper structures in the eye, potentially leading to progression of diabetic retinopathy or the development of macular edema. For this reason, not only success on the day of surgery but also long-term retinal follow-up for at least one year is central to treatment.
Q. I’m considering a multifocal lens—what should I pay extra attention to if I have diabetes?
Because multifocal lenses split light, their advantages are maximized when the retina is healthy. If diabetic retinopathy or macular edema is present, contrast sensitivity may decrease, so it is advisable to take a conservative approach with an ophthalmologist based on fundus exam results.

So far, we have reviewed the key criteria that patients with underlying diabetes should consider when planning cataract surgery. The main points this article aims to deliver are as follows.
First, a fundus exam to determine whether decreased vision is due to cataract alone or accompanied by retinal problems should come before the decision for surgery.
Second, do not jump to conclusions about surgery based on a single blood sugar value; instead, you should be evaluated comprehensively for overall systemic condition and the feasibility of coordinated care.
Third, leaving the operating room is not the end—one year of postoperative retinal follow-up is the final gateway to protecting functional vision.
If test results show that the retina is relatively stable, you can discuss a specific surgical schedule and lens selection with your medical team. Conversely, if macular edema is observed as active, it is a safer sequence to treat the retina first and build a stable foundation. Safe visual recovery begins with understanding the true condition of your eyes, so we encourage you to check each step carefully.
Sources
- Korea Disease Control and Prevention Agency (KDCA), guidance materials on diabetes management and complications (regular eye examinations) (SSOT citation)
- Journal of Korean Medical Science (JKMS), Trends and barriers in diabetic retinopathy screening (Korea NHANES 2016–2021), 2024
- American Journal of Ophthalmology, Incidence and progression of DR after cataract surgery: systematic review/meta-analysis, 2025
※ The copyright for all content on this blog belongs to medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.
Recommended reads
