
The growth phase is the "first opportunity" to guide jawbones in the right direction. However, even if you missed this window, modern orthodontic technology has opened a "second opportunity" that relies less on surgery. This guide helps you understand both opportunities and find the right path for you or your child today.
"I'm worried my child's jaw keeps sticking out."
"I heard adults need surgery to fix their bite."
These concerns are familiar. In orthodontics, the "growth phase" is indeed advantageous because the bones are still developing. However, there is no need to assume it is too late just because you are an adult.
The scope of non-surgical approaches has expanded significantly, and many techniques have been developed to reduce reliance on surgery.
This article covers the ideal value of early orthodontics and the innovative possibilities of adult orthodontics, helping you wisely seize these two critical opportunities.
1.The 'First Opportunity': Why is the Golden Time Beneficial?

The "Golden Time" is crucial because it is the first opportunity to utilize a child's jaw growth potential. During this period, we can improve skeletal imbalances themselves. The main goal focuses on balancing the jaw and face (skeletal harmony) rather than just aligning teeth.
What do we do?
We apply forces (orthopedic forces) to guide the jawbone to grow correctly. This force induces bone remodeling, increasing the likelihood of avoiding surgery in adulthood and reducing the duration and difficulty of Phase 2 treatment.
How does it work?
It typically proceeds in a two-step process if needed: Phase 1 (Skeletal/Space Management) → Observation (Monitoring Growth) → Phase 2 (Tooth Alignment). Often, setting the foundation in Phase 1 makes Phase 2 much simpler.
2.The 'Second Opportunity': What If I Missed the Timing?

"Is it too late if I missed the growth window?" The conclusion is: No.
While adults have finished growing, making skeletal changes difficult, various clinically established techniques like skeletal anchorage (OMI) now allow for precise and predictable tooth movement.
Additionally, MARPE (Miniscrew-Assisted Rapid Palatal Expansion) has established itself as a representative non-surgical alternative for expanding the upper jaw in adults without invasive surgery.
Key Non-Surgical Technologies
- Miniscrews (Skeletal Anchorage, OMI): Instead of using teeth as anchors, tiny screws are temporarily placed in the jawbone to create a solid support point. This significantly reduces unwanted movement of other teeth, allowing only the target teeth to move precisely. It serves as a non-surgical alternative for cases that previously required surgery, such as reducing protrusion or adjusting canted occlusal planes.
- MARPE (Non-Surgical Palatal Expansion): This method uses the force of miniscrews to gradually separate the mid-palatal suture (the seam of the roof of the mouth) without surgical incision. It has increased the possibility of improving narrow upper jaws without the traditional surgical procedure (SARPE).
Note: Severe skeletal malocclusions (e.g., severe Class III underbite) may still benefit more from surgery. The scope of non-surgical possibilities is determined through precise diagnosis.
3.What is the Fundamental Difference?
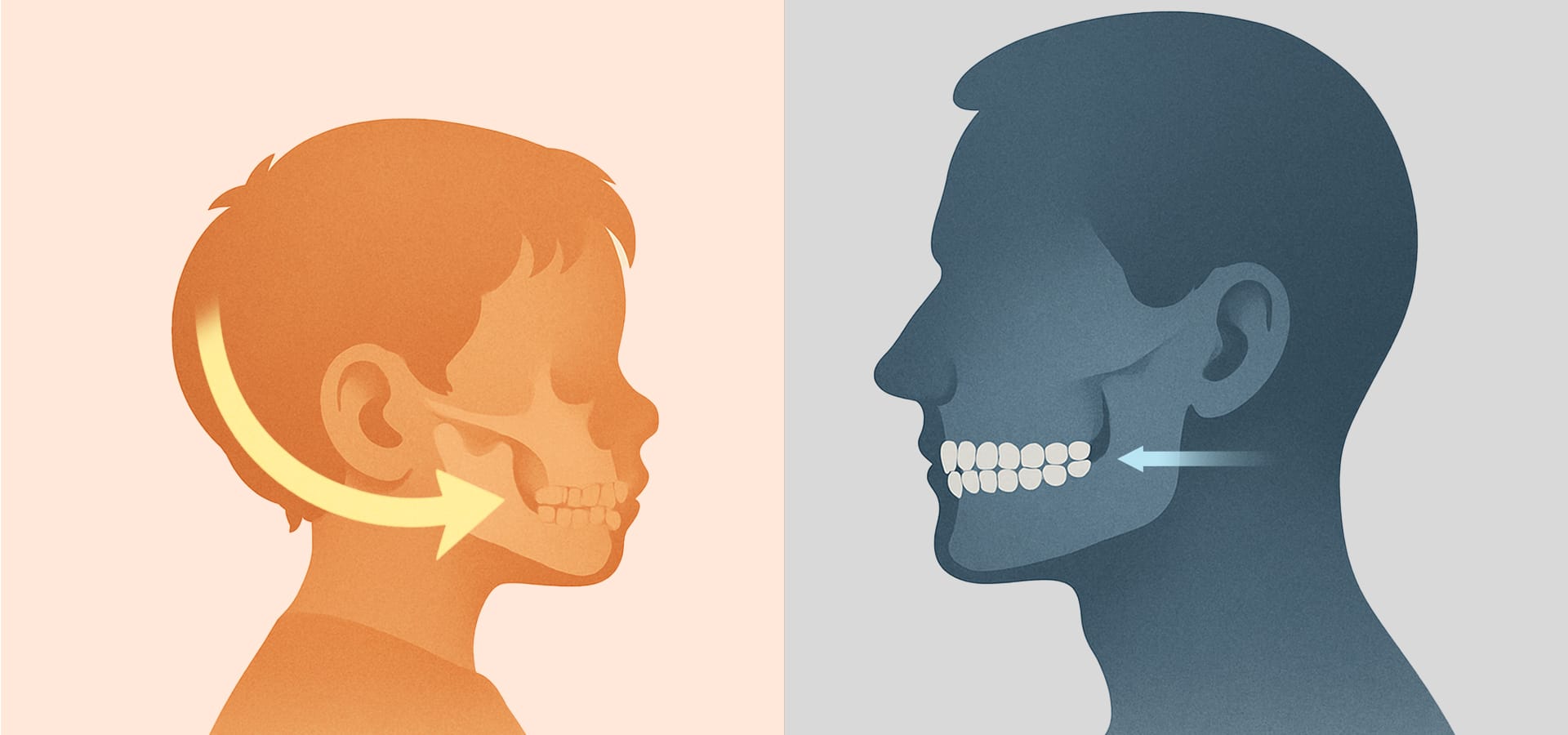
The core differences lie in the "scope of treatment" and the "source of force." Early treatment can partially control growth direction, while adult treatment focuses on precise tooth movement within a completed bone environment.
| Feature | Growth Phase (Kids) | Adult Phase |
| Target | Jaw growth direction control + Tooth movement | Precise tooth movement |
| Tools | Growth modification appliances (Orthopedic) | Miniscrews (TADs), Braces, Aligners |
| Goal | Skeletal balance & Space creation | Functional recovery + Esthetic improvement |
| Extraction | Non-extraction more likely | Extraction relatively common |
| Environment | Flexible bone (Easy to change) | Dense bone (Harder to change) |
Adults prioritize aesthetics and convenience due to social reasons, leading to widespread use of clear aligners and lingual braces. The goal is a composite improvement of both function (chewing, TMJ stability) and aesthetics through precise control.
4. Appliances, Techniques, and Latest Trends

Orthodontic appliances and methods are clearly distinguished by age group goals.
Growth Phase Appliances
Orthopedic appliances that induce bone remodeling (like Face Masks, Headgear) and removable functional appliances are mainly used. These aim for skeletal stabilization until growth is complete (Phase 1), usually followed by Phase 2 to align permanent teeth.
Adult Appliances
Besides fixed metal/ceramic brackets, Clear Aligners (e.g., Invisalign) and Lingual Braces are highly popular. Clear aligners are preferred for their hygiene and aesthetics but are also used for teens depending on the case.
Skeletal Anchorage (OMI & MARPE) has become a standard protocol to lower surgical reliance. While miniscrews are primarily used to overcome adult skeletal limitations, they are also used as auxiliary anchors in late adolescence.
Current Trends
- Increase in Adult Patients: One in three orthodontic patients globally is now an adult. Reports show a rise in patients over 40 seeking treatment.
- Enhanced Early Screening: Both the KAO and AAO recommend the first screening around age 7.
- Spread of Non-Surgical Methods: Technologies like MARPE and OMI have proven their safety and effectiveness in international journals, becoming standard treatments to reduce the need for surgery.
5.Treatment Duration & Cost: What’s the Real Burden?

For patients and guardians, the practical burden—duration, cost, and daily inconvenience—is as important as success.
| Aspect | Growth Phase (2-Stage) | Adult Phase (Single Stage) |
| Total Duration | 3~5 Years (Includes Phase 1, Observation, Phase 2) | 1.5~3 Years (Continuous) |
| Cost Timing | Staged (Phase 1 paid, then Phase 2 later) | Fixed at initial consultation |
| Payment | Installments per stage or lump sum for Phase 1 | Total lump sum or monthly plans |
| Predictability | Low — Depends on growth changes | High — Clear planning & outcome |
While skeletal anchorage or MARPE may add initial costs for adults, they can be cost-effective in the long run if they eliminate the need for hospital-based jaw surgery and recovery time.
6.Frequently Asked Questions (FAQ)
Q. If Phase 1 is done, is Phase 2 absolutely necessary?
Phase 1 aims for skeletal stability and space. If successful, Phase 2 might not be needed or could be very simple. However, Phase 2 is usually recommended to fine-tune the bite and alignment. The specialist will decide during the observation period.
Q. Can adults achieve functional goals beyond aesthetics?
Yes. Adult orthodontics treats functional goals like restoring chewing efficiency and TMJ stability as critically as aesthetics. Straight teeth also lower the risk of gum disease and cavities, playing a vital role in long-term oral health.
Q. Will my teeth move back after treatment?
Teeth have a tendency to return to their original position (relapse). Wearing retainers is a lifelong task to prevent this. Since adults have more significant periodontal changes, regular monitoring is even more critical.
Q. When is the best time for a consultation?
Now is the best time. For children, we recommend age 7. For adults, an accurate assessment of your current condition is more important than age. Especially if you have functional issues like TMJ pain, now is the optimal time.

Orthodontic treatment is about the harmony of timing and method. While the "Golden Time" of growth is still advantageous, the advancement of standardized non-surgical techniques has widened the options for later stages. Finding the best method for your current condition is the first step toward a lifelong smile.
Sources
- Korean Association of Orthodontists (KAO). (2024). Recommendation for First Check-up at Age 7 & Early Orthodontic Guide.
- American Association of Orthodontists (AAO). (2023). Age 7 Orthodontic Check-up & Adult Orthodontics Overview.
- Kang, S. H., Kim, J., & Lee, D. (2024). Miniscrew-assisted rapid palatal expansion in adolescents and adults: A scoping review. Journal of Clinical Orthodontics, 58(3), 123–134.
※ The copyright for all content on this blog belongs to Medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.
Recommended reads
