
A child’s malocclusion is not only an appearance concern—it can affect speech, breathing, and even school performance and self-esteem. This guide explains why early orthodontic care matters and helps parents understand the golden window for treatment and practical management points.
Parents often feel anxious about small changes.
“My child’s front teeth don’t meet properly.”
“They sleep with their mouth open—should I be concerned?”

These worries are common. On the surface, they can look like harmless habits, but there may be underlying issues with jaw growth and how the teeth fit together (occlusion).
If these early signals are missed, treatment later may become more complex—sometimes involving extractions or even surgery.
This article explains why growth-phase orthodontics matters, what can sometimes be addressed without surgery, and what parents can check and manage right now.
1.Why is malocclusion a problem for children?
Malocclusion refers to a condition where the upper and lower teeth do not fit together properly. In children, malocclusion can affect more than just tooth alignment—it may influence overall growth and health in several ways.
1) Speech concerns

- An open bite (when the upper and lower front teeth do not touch) can make sounds like “s,” “j,” and “ch” less clear.
- This may contribute to delayed speech development or teasing by peers, which can affect self-esteem
2) Breathing and facial development
- Mouth breathing (breathing through the mouth instead of the nose) may contribute to a longer facial pattern sometimes described as an 'adenoid-type face.'
- Reduced oxygen delivery during sleep can negatively affect concentration and academic performance
3) Psychological and social impact

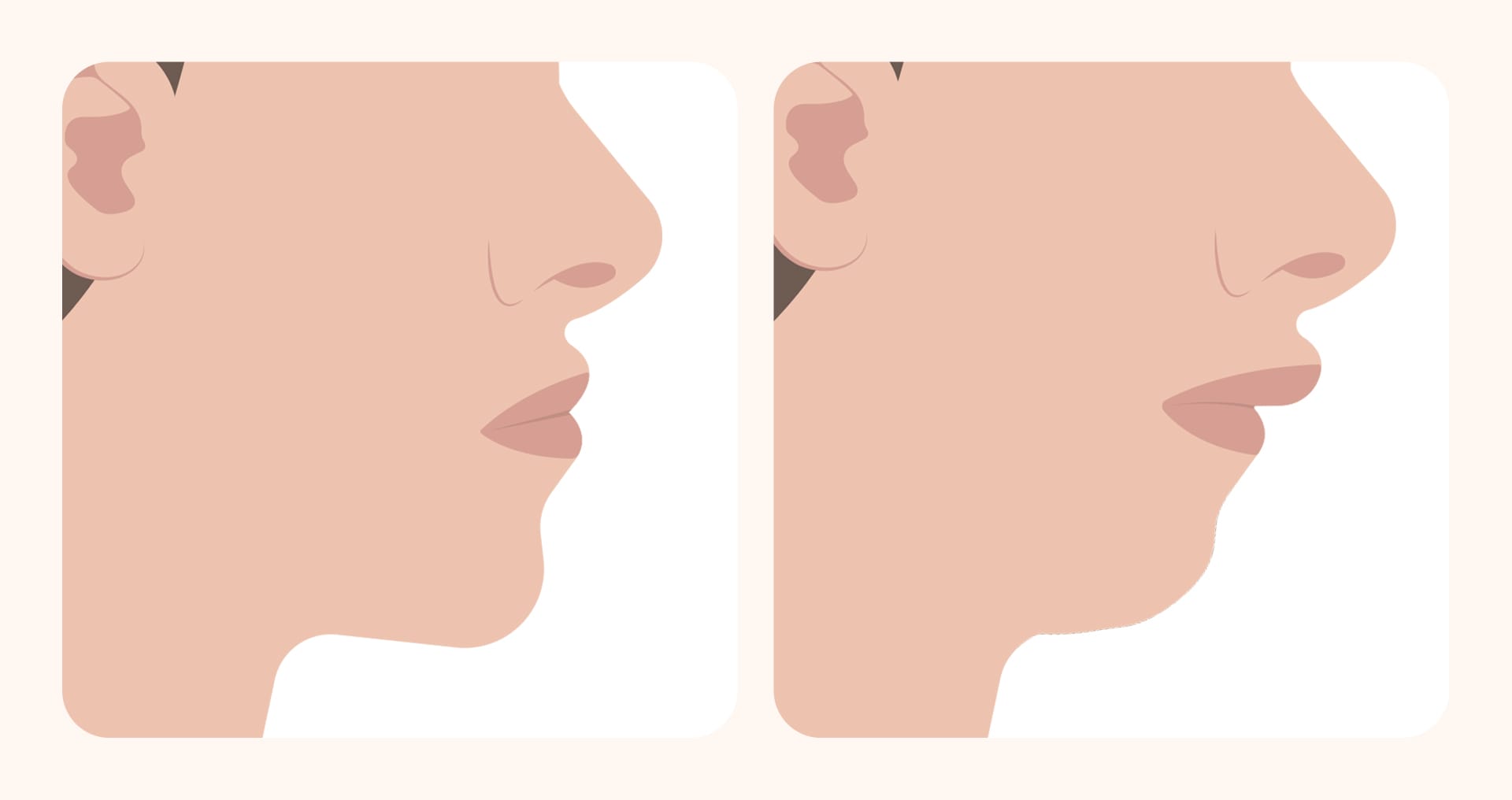
Changes such as protrusive lips or a receding chin can make a child hide their smile and may interfere with social confidence and development.
2.Why is early orthodontics called a “golden time”?
During childhood—especially the elementary school years (roughly ages 6–12)—the jawbones are still growing and more adaptable. This is often described as the golden window for orthodontic and jaw-growth guidance.
During this period, orthodontic appliances and habit correction can help guide the direction of jaw growth and reduce underlying contributors to malocclusion, which may lower the likelihood of needing extractions or surgery later.
If this window is missed, the jawbones become more stable, and adult orthodontics can become more complex. Extractions or jaw surgery may be considered, and both treatment time and burden can increase.
That is why growth-phase orthodontics is often described as a key opportunity to address malocclusion more efficiently and effectively.
[Growth-phase vs adult orthodontics]
| Category | Growth-phase orthodontics | Adult orthodontics |
|---|---|---|
| Timing | Ages 6–12 (mixed dentition) | After growth is complete |
| What can be addressed | Jaw growth + tooth alignment | Mainly tooth alignment |
| Need for surgery | Lower (may help prevention) | Higher (extractions/surgery more likely) |
| Typical duration | About 1–2 years on average | About 2+ years on average |
3.Are there non-surgical examples similar to my child’s case?
The appliances and plan depend on your child’s condition, but many growth-phase malocclusions can be treated with non-surgical methods.
Below are a few representative examples parents often ask about:
1) Child with open bite — removable appliance
- A child may have trouble biting through noodles or may speak less clearly.
- Tongue-thrusting habits can be a contributor, so treatment may combine a removable appliance with habit correction.
- With consistent wear, speech can improve and the front teeth may come back into functional contact.
2) Child with mouth breathing — palatal (arch) expansion
- If a child sleeps with their mouth open or shows a tendency toward a longer facial pattern, mouth breathing may be involved.
- In such cases, an arch expansion appliance may be used to widen a narrow upper jaw.
- As the upper jaw widens, airway space may improve and the tongue may return to a more stable resting position, helping the habit shift toward nasal breathing
3)Teen with protrusive lips — clear aligner treatment (Invisalign First)
- Some children struggle to keep lips closed comfortably or worry about a protrusive side profile.
- Pediatric clear aligner systems such as Invisalign First may be used to guide growth and improve alignment.
- With consistent wear, appearance can improve and children may regain confidence.
4.What parents can do: key management points

Successful treatment doesn’t happen through a child’s effort alone. A parent’s support and consistency can make a significant difference.
- Manage wear time
- Removable appliances or clear aligners often require 14+ hours per day to be effective.
- Help your child remember, and talk regularly about why consistent wear matters.
- Support hygiene
- Appliances should be cleaned daily to prevent bacterial buildup.
- Teach the correct method and help make it a routine.
- Correct harmful habits
- Thumb sucking or sleeping with the mouth open can reduce stability of results.
- Instead of scolding, encourage gradual habit change in a supportive way.
- Attend follow-ups and offer encouragement
- Regular visits are essential to keep treatment on track.
- Praise and encouragement help your child stay motivated.
5.Self-check checklist

Does your child do any of the following? Use this checklist as a quick screening tool.
[Self-check checklist]
| Checklist item | Possible signal |
|---|---|
| Trouble biting through noodles or frequent drooling | Possible open bite |
| Mouth open during sleep or heavy snoring | Possible mouth breathing / long-face tendency |
| Lisping or unclear pronunciation | Possible open-bite speech issue or tongue habit |
| Protrusive front teeth and difficulty closing lips | Possible protrusion |
| Chin shifts to one side when smiling or chewing | Possible crossbite / bite imbalance |
If two or more items apply, the pattern may be more than a simple habit and could signal malocclusion.
For example, difficulty biting noodles may suggest an open bite, and sleeping with the mouth open may suggest mouth breathing. If you notice concerning signs, consider consulting a professional.
6.Frequently Asked Questions (FAQ)
Q. When should my child get their first orthodontic evaluation?
A first evaluation is often recommended around age 6–7, when the first permanent teeth erupt. Even without obvious symptoms, checking jaw and tooth growth at this stage can help avoid missing the right timing for treatment.
Q. Is growth-phase orthodontics always necessary?
If the issue is only mild tooth alignment, orthodontic treatment as an adult may still be possible. However, jaw-bone patterns such as an underbite tendency (skeletal malocclusion) can make growth-phase treatment especially important. Since growth-phase jaw guidance is time-limited, it’s wise to consult an orthodontic professional.
Q. Will orthodontic treatment be very painful for my child?
In the first few days after starting an appliance, your child may feel pressure or soreness. This is a common part of teeth adapting to change and often improves quickly. If discomfort is significant, soft foods and professional guidance can help.
Q. Can teeth shift again after orthodontic treatment?
Yes. Additional growth during adolescence or later eruption of wisdom teeth can contribute to relapse. Wearing retainers and attending regular follow-ups are important for long-term stability.

Your child’s dental concerns are not “just cosmetic.” Malocclusion can affect speech, breathing, confidence, and overall quality of life. In particular, ages 6–12 can be a golden window that may help reduce the chance of surgery later. A parent’s attention can change a child’s future. If you recognize any of the warning signs discussed above, consider seeking a professional evaluation.
Sources
- Korean Association of Orthodontists. (2022). Pediatric & Adolescent Orthodontic Clinical Guidelines. Korean Journal of Orthodontics, 52(3), 145–160.
- Korean Academy of Pediatric Dentistry. (2021). Recommendations for Early Orthodontic Treatment in Children. Journal of the Korean Academy of Pediatric Dentistry, 48(4), 321–332.
- Proffit, W. R., Fields, H. W., & Larson, B. (2021). Contemporary Orthodontics (7th ed.). Elsevier.
※ The copyright for all content on this blog belongs to Medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.
Recommended reads
