
This post summarizes the causes of shoulder dislocation instability and the criteria used to judge the risk of redislocation. If you feel afraid your shoulder might “pop out” when throwing a ball, check what that fear may be signaling about structural damage—and when surgical vs. non-surgical options may be considered.
“I get scared my shoulder will pop out when I throw a ball, so I stop.”

Many men in their 20s and 30s come to the clinic with this concern. This is not simply “being weak” or getting scared for no reason. It may be your body’s protective response to avoid further injury, so a proper evaluation of the underlying cause can be helpful.
1. Anxiety when throwing—just soreness or weak muscles?

When you throw a baseball or serve in tennis, you typically move your arm out to the side and rotate it outward (abduction and external rotation).
If, in that position, you feel a clunking sensation or a sudden fear that the shoulder might slip out, this is medically described as “apprehension.” It’s easy to mistake this for simple deconditioning or mild muscle soreness.
However, this fear is not merely psychological hesitation. The shoulder joint can be
compared to a door and its frame. The door frame (glenoid) and the hinges (ligaments) must be intact for the door (humeral head) to open smoothly. When the structure is damaged, opening the door wide can create a loose, unstable feeling—like the door might come off.
In other words, repeatedly “freezing” during a specific movement is a classic clinical clue suggesting anterior instability. Even if the pain does not look severe on the surface, it may indicate that the bones and soft tissues inside the joint are no longer tracking normally. That is why physical examination findings should be interpreted together with imaging.
2. A shoulder that dislocated once—why is redislocation risk especially high in younger
people?

In older adults (often 50+), a shoulder dislocation is relatively more likely to be accompanied by a rotator cuff tear. In contrast, men in their 20s–30s often have relatively strong tendons, but the soft tissues and even the bone that stabilize the joint may be damaged—so repeated redislocation is reported more frequently.
Younger people tend to be more active and are more likely to participate in contact or high-demand overhead sports. Using the same analogy, the harder you slam a door, the faster a damaged hinge becomes loose. This high activity level can place ongoing stress on the joint.
Even if it was a first-time dislocation, repeated episodes can accumulate structural damage such as bone loss. Therefore, the younger you are—and the more strongly you want to return to sports—the more important early evaluation becomes.
✅Signs that may indicate higher recurrence risk (self-check)
- You are a man in your 20s–30s and continue contact or overhead sports.
- The “about to slip out” sensation repeats when you abduct the arm and rotate it
outward/back. - You have had shoulder dislocation or subluxation two or more times.
- Because of apprehension, you start avoiding certain sports movements on your own.
3. Is the bone worn down, or is the ligament torn? Criteria that change the treatment plan
When deciding the direction of treatment for shoulder instability, the first step is confirming what is damaged—and how much. In the clinic, the condition of three major structures is commonly used as the basis for decision-making.
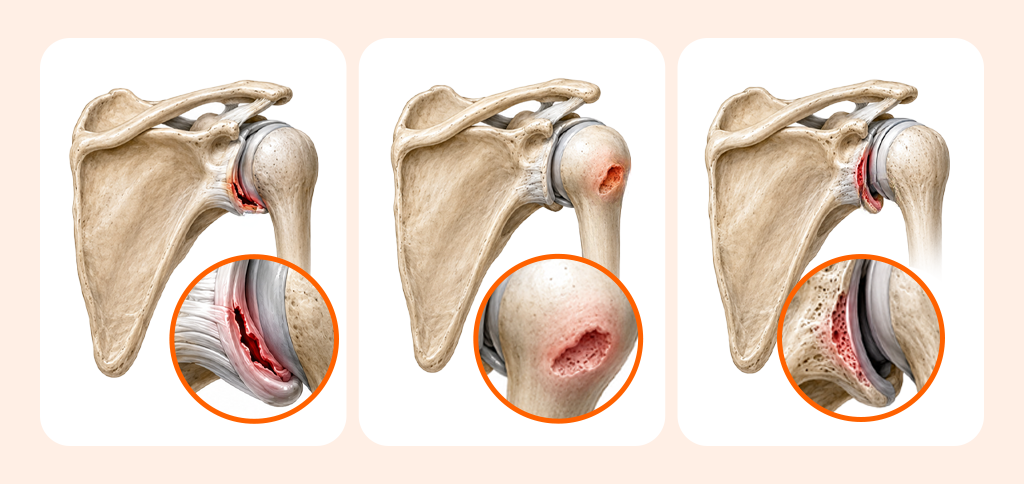
| Lesion | What is damaged? | Significance in Instability |
|---|---|---|
| Bankart Lesion | Labrum and capsule complex (Anteroinferior) | If the edge of the door frame (labrum) is torn, the door can easily slide forward. |
| Hill-Sachs Lesion | Impaction defect of the humeral head | If a dent is left on the corner of the door (humeral head), the risk of 'catching' at certain angles may change. |
| Glenoid Bone Loss | Bone loss of the anteroinferior glenoid | If the door frame (glenoid) itself is worn down, the support decreases, which may alter the method of stabilization. |
A ligament tear alone is like a hinge that has become loose. But bone wear is like the door frame itself breaking.
If the frame is broken, even a strong hinge won’t stop the door from wobbling again. To assess this, clinicians use the “On-track/Off-track” concept to analyze the risk of bony engagement.
If the analysis indicates On-track (no engagement risk), soft-tissue stabilization surgery may be discussed. If it is Off-track or the bone loss is substantial, a bony augmentation procedure may also be considered—so individualized assessment is essential.
4. Surgery vs. non-surgical care: conditions that help determine the safer direction for
your situation

If your shoulder dislocated for the first time, there is no bone defect, and your daily life is the main priority, immobilization with a brace followed by rehabilitation may be favorable. With a non-surgical approach focused on stepwise strengthening, you may aim to improve dynamic stability.
However, the situation can be different if there is meaningful bone wear or if returning to high-intensity sports is essential. Early surgical stabilization to reduce redislocation risk may be discussed.
If the issue is primarily ligament/soft-tissue damage, arthroscopic Bankart repair is often considered. If bone loss is large, a bony procedure involving bone grafting/augmentation (such as a Latarjet-type procedure) may be appropriate. When a Hill-Sachs lesion is clinically significant, additional arthroscopic adjunct procedures may also be reviewed.
✅Helpful items to check before a consultation
- Does the fear of “it might slip out” recur with specific movements?
- Regardless of pain, are you avoiding certain sports movements on your own?
- After the shoulder came out, has your athletic performance failed to return to your previous level?
5. Returning to sports after surgery: why “function” matters more than a simple timeline

After surgery, it’s easy to assume that once a certain number of months pass, you can automatically return to sports. But restoring the bone and ligaments is only part of the process. The rest depends on the quality of rehabilitation—regaining range of motion and rebuilding dynamic strength.
During the period of brace use, the muscles around the shoulder naturally stiffen and weaken. Trying to “loosen everything” all at once can actually increase the risk of reinjury. Rather than focusing on a vague target like “six months,” it is important to meet functional recovery criteria such as the following:
- Step 1: Restore normal, pain-free range of motion for daily activities
- Step 2: Achieve strength symmetry compared with the healthy shoulder
- Step 3: Regain functional ability to perform sport-specific movements for your goal sport
- Step 4: Psychologically overcome fear during movement (kinesiophobia)
Rushing back before confidence is fully restored can disrupt overall body balance. For that reason, following a structured, step-by-step rehabilitation protocol coordinated with medical professionals is recommended.
6. Frequently Asked Questions (FAQ)
Q. My shoulder has dislocated once—how do you determine my risk of redislocation?
We assess this comprehensively based on age, the intensity of sports activity, and imaging findings such as the degree of glenoid bone loss and labral injury. In particular, for active patients in their 20s–30s, structural damage may be present, so a detailed evaluation is often recommended.
Q. If I feel like it might “pop out” during exercise, which movements should I temporarily avoid?
Positions where the arm is raised and rotated outward (abduction and external rotation) can place strong stress on the anterior capsule. If apprehension repeats during a throwing motion or a tennis-serve position, it’s best not to force the movement and to seek evaluation from a clinician first.
Q. When are Bankart repair and Latarjet surgery considered?
If the damage is mainly to stabilizing soft tissues (such as ligaments and the labrum), arthroscopic Bankart repair—suturing the injured tissue—may be appropriate. If repeated dislocations have led to meaningful loss of bone itself (glenoid bone loss), a bony augmentation procedure such as Latarjet may be more advantageous.
Q. When should I seek medical care urgently for shoulder instability?
If an acute dislocation is suspected, or if there is severe deformity or symptoms involving nerves or blood vessels, prompt emergency evaluation and reduction should come first. Even after reduction, if apprehension persists during sports movements, it is safer to undergo a detailed diagnostic workup before larger structural damage accumulates.

The most important part of treating shoulder instability is clearly defining your current condition. You need to determine whether it is simply ligament laxity or whether bone damage is accumulating. If bone wear is progressing, leaving it unaddressed can lead to larger structural changes.
That hesitation when throwing is not your fault, nor is it merely psychological weakness. It may be a reasonable “brake” your body applies to protect the joint. Rather than ignoring the signal, consider working with your medical team to design the safest treatment plan based on the extent of damage and your return-to-activity goals.
Sources
- Ministry of Health and Welfare, National Health Information Portal, Shoulder joint dislocation and instability, 2023
- Seoul National University Hospital Medical Information, Shoulder dislocation, 2023
- Cutteridge et al., First-time traumatic anterior shoulder dislocation surgery vs nonoperative (meta-analysis), Shoulder & Elbow, 2025
※ The copyright for all content on this blog belongs to medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.