
This post lays out clear criteria for distinguishing between vision decline due to cataract & presbyopia and true ophthalmic emergencies that have a “golden time” for evaluation and treatment. The goal is to reduce anxiety when sudden symptoms occur and help you decide when you should head to an eye clinic.
“Up until yesterday I could see fine, but today I suddenly can’t see out of one eye—I’m terrified.”

Many people say this in the exam room, visibly shaken. If half the world suddenly goes dark, anyone would feel frightened and confused. In situations like this, people who have previously been diagnosed with cataract & presbyopia often worry that their presbyopia or cataract has worsened and tend to “wait a few days and see.”
Clinically, however, cataracts do not typically take vision away overnight. If one eye becomes difficult to see out of over a short period of time, it may be an emergency signal pointing to problems involving the retina, optic nerve, or blood vessels. In this article, we’ll organize practical criteria to help distinguish cataracts from other ophthalmic emergencies.
1. If your vision dropped within a day, why it’s unlikely to be “cataracts”
Imagine your eye as a house. A cataract is like a light bulb that gradually reaches the end of its lifespan over years, making the light dimmer and dimmer. But if a light that worked fine yesterday suddenly goes out today, it’s not because the bulb “wore out overnight”—it’s more like the circuit breaker tripped or there’s a wiring problem. A rapid drop in vision within a day may be separate from cataract progression.
Many people who already have a cataract diagnosis end up attributing any vision decline to cataracts. But cataracts typically progress very slowly and without pain. Even if you’ve had cataracts for a while, a sudden change in vision should raise the possibility that something acute is happening—related not to the lens, but to the retina, optic nerve, or intraocular pressure.
If your vision has gradually become hazier over months to years, suspecting cataract progression is reasonable. However, if vision drops sharply within hours to a day, the approach changes completely:
If the field of view darkens without pain, retinal conditions such as retinal vascular occlusion or retinal detachment should be considered. If severe eye pain occurs along with headache and nausea/vomiting, a sudden spike in eye pressure—such as acute angle-closure glaucoma—should also be considered.
2. Floaters and flashes: how to tell simple aging from a retinal emergency

Floaters (seeing dust-like specks or strands drifting in your vision) and flashes (brief bursts of light, often more noticeable in the dark) are common in middle-aged and older adults. But if these symptoms start to look different from your usual pattern, caution is needed. It can be like wallpaper (the retina) about to peel—while the sensor starts malfunctioning and gives off subtle warning signals.
Studies report that among patients who visit the hospital for new floaters or flashes, some are found to have a retinal tear. It’s easy to dismiss this as fatigue, but if a tear progresses to retinal detachment—where the retina begins to separate—it can significantly affect vision. In particular, if part of your visual field starts to become blocked as if a black curtain is coming down, it may suggest a retinal tear or detachment, and a dilated fundus exam may be needed.
If you have high myopia, a family history of retinal detachment, or a personal history of retinal detachment/tear in the other eye, you may need faster evaluation even with similar symptoms.
If you simply notice one or two more floaters than usual, it may be reasonable to monitor through routine checkups. But if dozens appear within a day, or if a visual field defect accompanies them, getting prompt testing may help preserve vision depending on the cause.
✅Retinal emergency suspicion checklist
- A sudden, explosive increase in floaters (dozens or more)
- New flashes in the dark, or flashes that are getting worse
- One edge of the visual field looks blocked, like a black curtain
- Symptoms change rapidly over hours to one day
- High myopia, family history of retinal detachment, or prior personal history
3. When headache and vomiting mean “ophthalmology first,” not internal medicine

When eye pain occurs together with headache, reflux & heartburn, and vomiting, many people go first to the ER’s internal medicine or neurology services. They assume it’s indigestion or a brain problem. But it’s important to consider that these can be symptoms of acute angle-closure glaucoma, caused by a sudden rise in intraocular pressure.
Acute angle-closure glaucoma occurs when the drainage pathway for aqueous humor (the fluid inside the eye) suddenly becomes blocked. It’s like a clogged pipe in a house: when water pressure rises abnormally, the strain doesn’t stay localized—it affects the whole system. When eye pressure spikes, it can cause not only eye pain but also severe headache and nausea by triggering nerve pathways.
If you only have simple indigestion or a headache and your vision is completely unaffected, internal medicine may be appropriate. But if you have severe headache and vomiting along with a red eye, deep aching eye pain, and halos/glare around lights, an eye exam may be needed. In that situation, it’s advisable to seek care where intraocular pressure can be measured.
4. Sudden vision loss without pain: when you may need systemic vascular evaluation too
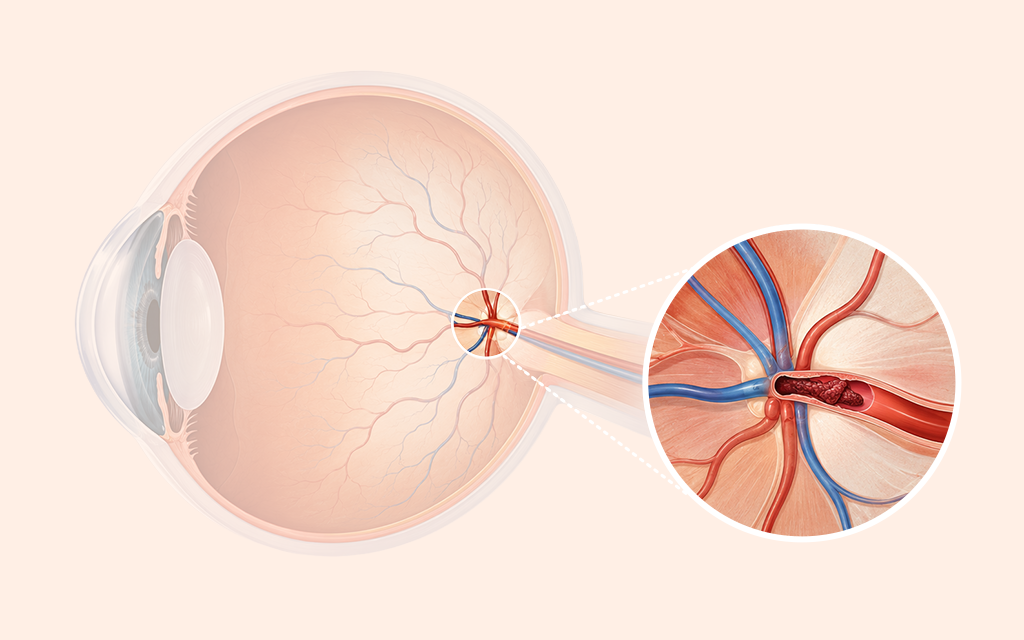
It’s easy to think something is only dangerous if there’s bleeding or pain. But one acute condition can occur quietly, with no pain at all: central retinal artery occlusion (CRAO). It’s like the main power line feeding a house being cut—suddenly everything goes dark even though the light bulbs themselves are fine.
When the artery supplying blood to the retina is abruptly blocked by a thrombus (blood clot), a person may lose vision in an instant without feeling pain. The key point is that an eye vessel blockage can suggest the need to discuss evaluation of systemic blood vessels as well—such as cerebral or cardiovascular circulation. It may reflect overall vascular health.
If your eye is painful, red, and your vision is dropping, acute glaucoma may come to mind first. But if vision disappears like a switch being turned off—without pain or redness—vascular occlusion should be considered. In such cases, it may be advantageous to seek an emergency medical facility where ophthalmic evaluation and systemic evaluation can be coordinated.
✅Painless sudden vision loss checklist (including vascular causes)
- No eye pain and no red eye at all
- Sudden loss of vision in one eye within minutes to hours
- Systemic symptoms along with eye symptoms (e.g., limb weakness, slurred speech)
- History of hypertension, diabetes, or cardiovascular disease
5. If pain suddenly starts in an eye after surgery, what should you check?
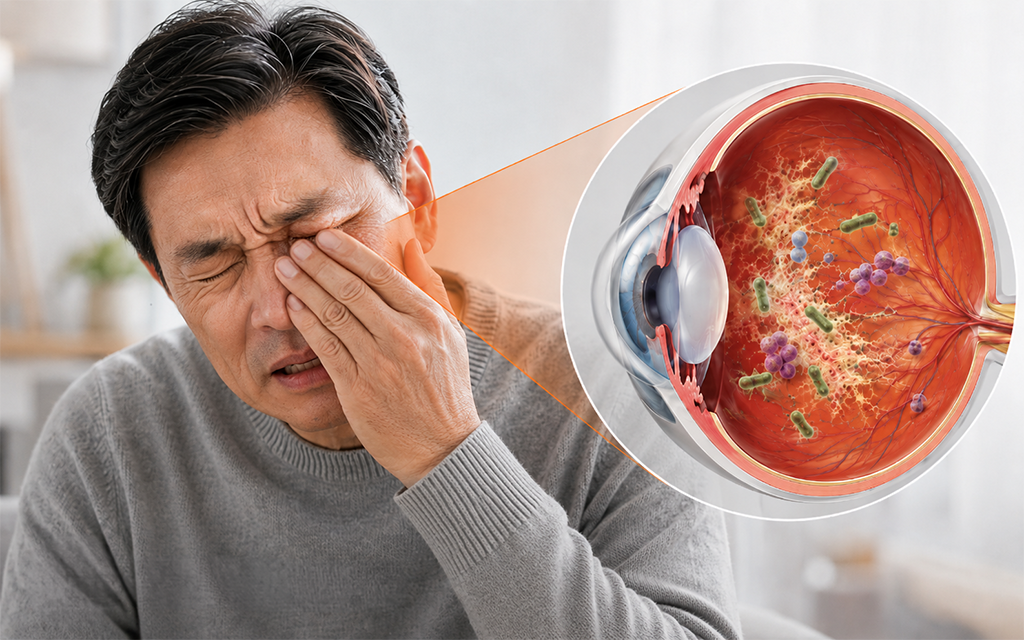
Even after a successful cataract surgery, there is an exceptional situation that requires caution: postoperative endophthalmitis. You can think of it as replacing an old light bulb with a new one—only to have sparks of infection ignite deep inside the eye not long afterward.
It is rare (fewer than 1 in 1,000), but once an infection begins inside the eye, inflammation can progress quickly. After cataract surgery, it’s common for anyone to experience mild foreign-body sensation or light sensitivity, so people sometimes mistake early infection signs for a normal recovery process and endure the pain. However, without early, proactive evaluation, it can significantly affect vision.
Right after surgery, mild dryness/tightness or light sensitivity is usually managed by resting and using prescribed eye drops. Endophthalmitis most often appears acutely within one week after surgery, but in rare cases it can also present in a more slowly progressive form vnearly a month later. If the eye becomes sharply painful, red, and vision drops rapidly again, caution is needed. Because these may be warning signs of infection, it’s advisable to have the inside of the eye checked at the surgical clinic or a nearby medical facility.
6. Frequently asked questions (FAQ)
Q. My vision suddenly became blurry in one eye, but there’s no pain. Can I just wait and see?
No. Vascular conditions or retinal detachment can cause rapid vision loss even without pain. Lack of pain does not mean it’s safe. If your vision changed over a short period, an ophthalmic exam is needed to identify the cause.
Q. I think my floaters have increased—can they go away on their own?
Mild floaters related to aging may become less noticeable over time as you adapt. However, if floaters increase to dozens within a day or two, or if flashes accompany them, it may be a sign of a retinal tear. Rather than expecting natural recovery, confirming the cause should come first.
Q. If headache, vomiting, and a red eye happen together, which department should I go to?
If severe headache and vomiting occur together with eye pain, it may not be simple indigestion or a brain disorder—it could be acute angle-closure glaucoma due to a sudden rise in intraocular pressure. If you have severe eye pain and redness, rainbow-colored halos around lights, and sudden blurring of vision, ophthalmology may be the priority.
Q. After symptoms start, when should I go to the hospital?
If the change wasn’t gradual over months but instead vision dropped sharply within hours to a day; if your visual field is blocked like a black curtain; or if severe eye pain occurs with headache and vomiting, it’s best to seek a facility that can provide ophthalmic care as soon as possible.
The key mistake to avoid when vision suddenly worsens or severe pain occurs is attributing it to “just being tired” and delaying your visit. Cataracts do not take vision away overnight. Behind a rapid change in vision, conditions that require differentiation—such as retinal detachment, an acute glaucoma attack, or vascular occlusion—may be present.
Because timing can matter depending on the cause, it’s better not to postpone evaluation if you have these symptoms. If any of the warning signs discussed above apply to you, consider visiting a medical facility where a fundus exam and intraocular pressure measurement are available. A prompt specialist assessment can help guide early response.
Sources
- Journal of the Korean Ophthalmological Society, Clinical features of delayed diagnosis in acute angle-closure glaucoma patients visiting the emergency room, 2020
- Korean Journal of Ophthalmology, Analysis of 113 cases of endophthalmitis after cataract surgery
- Stroke (American Heart Association), Management of central retinal artery occlusion: A scientific statement, 2021
※ The copyright for all content on this blog belongs to medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.
Recommended reads
