
The health of the retina is a medical area that’s difficult for patients to recognize in advance. This post explains why taking a close look at the retina before cataract surgery becomes a clear benchmark for setting realistic expectations about postoperative vision.
“After surgery, will my vision become clear again like it used to be?”

This is a question many patients commonly ask when they come to the clinic ahead of cataract surgery. It’s often because they believe cataracts are the only reason their vision has become blurry.
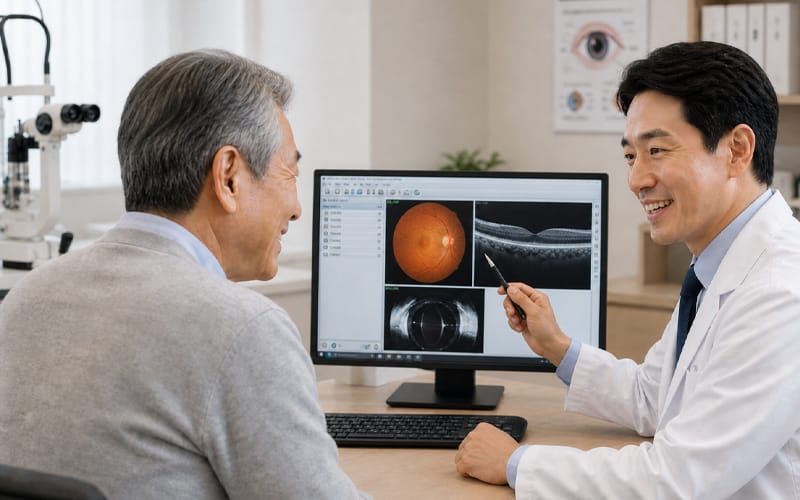
However, what clinicians pay the closest attention to before cataract surgery is the health of the “retina,” the inner part of the eye that ultimately receives visual information. By performing a detailed retinal evaluation before cataract surgery, we can confirm whether the foundation is healthy—so you can more comfortably anticipate clearer vision like before.
Now, let’s go over why it’s important to examine the retina carefully before cataract surgery.
1. Why replacing the intraocular lens alone may not be enough to restore vision
The structure of the eye works similarly to a high-performance camera. A cataract refers to clouding of the eye’s lens (the crystalline lens), like a camera lens becoming foggy. Cataract surgery is the process of replacing this cloudy lens with a clear artificial lens (an intraocular lens). Once the lens becomes clear, external light can enter the eye more effectively.
But what if the camera’s image sensor deep inside is damaged? Even if you replace the lens with an excellent one, the final photo can still come out blurry. In the eye, the retina and macula play the role of that sensor.
If conditions such as macular degeneration or diabetic retinopathy are also present, the outcome can be different. Even after the lens is replaced, visual recovery may be limited due to the sensor’s own constraints. Medically, it’s important to assess the “image sensor” status before surgery so that postoperative visual expectations can be set realistically.
2. When is an OCT needed even if the dilated fundus exam looks normal?
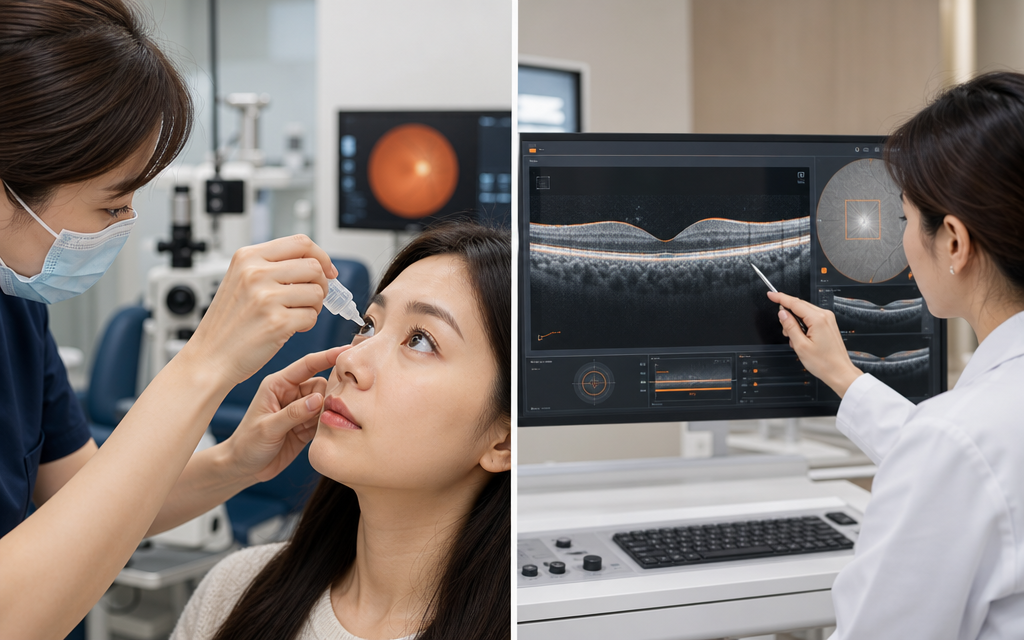
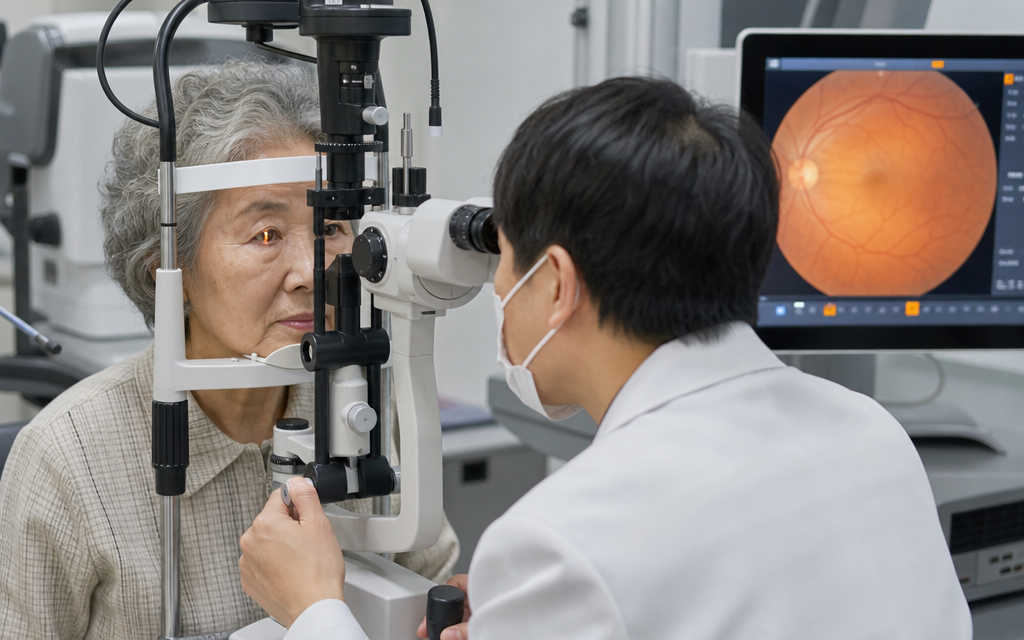
The most basic way to check the retina before surgery is a dilated fundus exam. After using eye drops to widen the pupil, the clinician looks into the back of the eye to check for overall retinal bleeding or obvious abnormalities. However, even if everything appears normal on the surface, it doesn’t always mean there is nothing to worry about. Looking only at the surface of a camera sensor is different from viewing its internal circuitry in cross-section. For this reason, a macular OCT may be performed depending on the situation.
[Comparison of key features by retinal test type]
| Category | Detailed Fundus Exam (Mydriatic) |
Macular OCT Exam |
|---|---|---|
| Primary Purpose | Direct observation of the overall retina | Cross-sectional visualization of macular structure |
| Key Findings | Hemorrhage/exudates, vascular changes, suspected tears | Macular edema, epiretinal membrane, boundary abnormalities |
| Limitations | Observation is limited if severe opacity is present | Image quality degrades if severe opacity is present |
According to published research, even among patients with a normal basic fundus exam, when a macular OCT is performed, latent lesions are found in roughly 13–22%. This percentage can vary depending on study design and population, but it is true that latent lesions are often reported in older adults or in patients with diabetes.
If you are around your 70s or have diabetes, the likelihood of hidden lesions is higher, so adding a macular OCT can be much more helpful for predicting prognosis. If there are no specific concerns, treatment can be planned based on the fundus exam.
✅Checklist: situations where an OCT may be considered
- Vision loss that seems relatively severe compared with the degree of cataract
- Distortion in the center of vision or a sense of visual “tightness”/pressure
- Older age (including around the 70s), or diabetes, or high myopia
- The macula is not clearly visible on the dilated fundus exam
3. Why retinal status is checked more carefully before surgery if you have diabetes
For people who have had diabetes for a long time, a more cautious approach is needed when planning cataract surgery. Diabetes affects blood vessels throughout the body, and the tiny blood vessels inside the eye are no exception. This can weaken retinal vessels and lead to diabetic retinopathy, which may involve bleeding and swelling. Cataract surgery itself is generally considered a relatively safe procedure, but inflammation can occur inside the eye during the surgical process and recovery.
Some studies have reported an increased risk of diabetic retinopathy progression after surgery. Therefore, it is safer to monitor retinal status more closely before and after surgery. If macular edema is significant before surgery or blood sugar control is poor, a different plan may be needed.
Depending on the condition, retinal treatment may be considered first and the timing of surgery adjusted. Based on the stage of diabetic retinopathy, anti-VEGF injections or laser treatment may be combined before surgery to stabilize the intraocular environment, followed by cataract surgery. On the other hand, if blood sugar is well controlled and the retina is stable, surgery can proceed as planned. Even so, in patients with diabetes, retinal changes may appear later after surgery, so closer follow-up than in the general population is often necessary.
4. Multifocal intraocular lenses: why “retinal status” comes before price
Choosing which intraocular lens to implant is often one of patients’ biggest concerns. Multifocal lenses, which many people choose today, work by splitting light. They divide incoming light so that both distance and near focus can be achieved. For vision to be clear, the retina must fully receive this divided visual information and transmit it to the brain.
What if there is subtle retinal disease or reduced optic nerve function? The damaged retina may not properly process the light passing through a multifocal lens. In such cases, symptoms like overlapping images or increased blur can feel more pronounced.
In these situations, choosing a monofocal lens that concentrates light into a single focal point can improve the predictability of postoperative vision. Conversely, if the retina is very healthy, a multifocal lens may be a favorable option. Lens selection should prioritize the health status inside the eye above all else.
✅Items to confirm during intraocular lens counseling
- Whether OCT is needed to differentiate subtle macular lesions that are difficult to confirm with a standard fundus exam alone
- Whether additional management is needed before and after surgery considering current underlying conditions (such as diabetes)
- Which lens type is likely to provide more predictable visual recovery based on retinal health
5. Two things to check if vision becomes blurry again after surgery
After cataract surgery goes well, some people experience blurred vision again as time passes. Many assume it is “posterior capsule opacification,” where cells grow on the membrane behind the lens. If it is posterior capsule opacification, vision can often be cleared relatively easily in the outpatient clinic with a YAG laser procedure.
However, it’s also important to consider that the cause may be changes on the “camera sensor” side—meaning the retina. With aging, macular degeneration may newly and gradually develop. For those who already have diabetes, there is also a significant possibility that retinal changes progressed quietly over time after surgery.
In particular, patients with high myopia and a long axial length can experience physical changes inside the eye. If new vision loss or a curtain-like visual obstruction appears, do not assume it is only posterior capsule opacification. It is very important to undergo a repeat fundus exam or OCT to identify the exact cause.
6. Frequently asked questions (FAQ)
Q. If my fundus exam is fine, is there a reason to add an OCT?
It is to evaluate subtle changes in the retinal nerve layers in a three-dimensional, cross-sectional way that may not be visible on the surface. If you are older or have diabetes, even when the fundus appears normal, latent lesions have been reported in roughly the 13–22% range on OCT. Additional testing can help improve prognostic accuracy.
Q. If I have diabetes, should I postpone cataract surgery?
Not necessarily. The decision depends on blood sugar control and whether macular edema is present. It may be more advantageous to treat macular edema first and proceed with cataract surgery once the condition is stable.
Q. What should I do if I develop floaters or flashes after surgery?
If you suddenly notice many more floaters, or see flashing lights in the dark, you should be cautious. In conditions such as high myopia, these can be signals of peripheral retinal changes, so a prompt, detailed ophthalmic evaluation is recommended.
Q. When is the best time to get a preoperative eye exam and consultation?
It’s best to visit an eye clinic without delaying once you start noticing visual discomfort. In particular, if you are older or have underlying conditions such as diabetes, it is safer to have your eyes checked promptly when you notice changes in vision.
Checking the retina and macula before surgery is not meant to complicate the care process. It is an essential step to find the right timing for surgery and the most suitable lens type for each patient. It helps establish a more accurate and safe basis for how well you may be able to see after surgery.
Even if you have underlying conditions or are older, you do not need to worry excessively. With a precise diagnosis and a treatment plan tailored to your current status, visual discomfort can be reduced in a steady and controlled way.
Sources
- Jae Ik Kim · Jong Hyun Oh, Long-term cumulative incidence and risk factors of epiretinal membrane after cataract surgery, Journal of the Korean Ophthalmological Society, 2021
- The Korean Retina Society, Guidelines for cataract surgery and retinal management in patients with diabetes, 2023
- American Academy of Ophthalmology (AAO), Cataract in the Adult Eye Preferred Practice Pattern, 2021
※ The copyright for all content on this blog belongs to medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.
Recommended reads
