
If your vision becomes blurry again after cataract surgery, it is often due to a natural structural change called posterior capsular opacification (PCO), rather than a failed surgery. Instead of worrying right away, it’s best to have a thorough eye examination to identify the exact cause and then choose safe treatment and follow-up care tailored to your eye condition.
“My vision has become cloudy again a few years after surgery—does that mean my cataract has come back?”

When vision becomes blurry again after cataract surgery, it’s natural to worry that something went wrong or that the cataract has returned. However, rather than feeling anxious without clear information, it’s important to calmly determine which structure inside the eye has become cloudy. This matters because recommended treatment and follow-up plans can differ completely depending on the cause.
When an ophthalmologist encounters this symptom, the first thing they typically assess is not surgical failure or “cataract recurrence,” but the condition of the thin membrane that supports the intraocular lens (IOL).
1. Why it may not be “cataract recurrence,” but posterior capsular opacification (PCO)
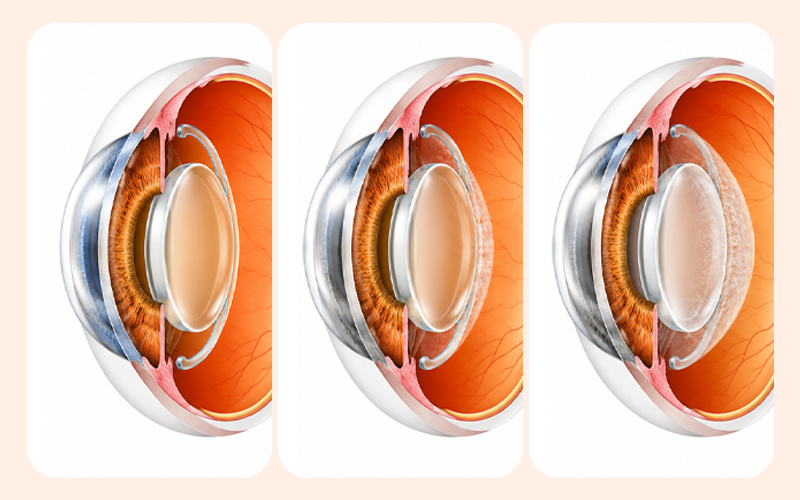
Posterior capsular opacification is a phenomenon in which the thin, transparent membrane left inside the eye after surgery (the lens capsule) gradually becomes cloudy. During cataract surgery, the cloudy natural lens is removed and replaced with a clear artificial lens. To secure the new lens firmly, the transparent back membrane—like clear plastic wrap (the posterior capsule)—is intentionally left in place.
Over time, tiny residual cells around the lens can proliferate or migrate. As a result, the previously clear membrane develops cloudiness, like frost forming on glass, and vision becomes blurry again. Medically, this is called posterior capsular opacification (PCO). Large-scale studies, including analyses of more than 500,000 surgeries in the UK, have confirmed that this is a relatively common change over time.
The most common misunderstanding is thinking, “The cataract that was removed grew back.” In reality, it is closer to a normal tissue-healing response inside the eye—similar to how a scar can form as a wound heals. In other words, it is not a “recurrence” caused by poor patient care or a botched surgery, but a structural change that can occur naturally.
2. Why are tests needed to distinguish posterior capsular opacification?
It can be risky to assume that blurry vision automatically means posterior capsular
opacification. Think of the eye like a camera: you need to determine whether the “lens” (posterior capsule) has fogged up, or whether the “sensor” (macula) or the “wiring” (retina, optic nerve) has a problem. Diagnostic testing is essential.
If the true cause is a retinal disease or glaucoma, and only the capsule is treated with a laser, vision will not clear. You can roughly gauge which side your situation resembles by noting the symptom patterns below.
| Signs Suggesting Posterior Capsular Opacification (PCO) First | Warning Signs Requiring Retinal or Optic Nerve Check |
|---|---|
|
• Gradual, progressive blurring of vision • Nighttime glare and reduced contrast sensitivity |
• Sudden flashes of light (Photopsia) • Part of the vision obscured, like a curtain drawing • Distorted central vision or a sudden increase in floaters |
Because posterior capsular opacification can sometimes be detected relatively early, it’s safer not to assume, “It hasn’t been that many years, so it can’t be that.” The safest approach is to have the eye examined directly with ophthalmic equipment to pinpoint the cause.
✅Symptom memo checklist before your visit
- When the blurriness started (gradual worsening vs. sudden worsening over a few days)
- Where symptoms occur (one eye only vs. both eyes)
- Whether there are additional symptoms such as glare, halos/starbursts, or flashes
- When you last had an intraocular pressure test and a fundus (retinal) exam
- Whether you have underlying conditions such as diabetes or hypertension, and when you last had a fundus exam
3. What is YAG laser (laser treatment)?
If a detailed exam clearly confirms that posterior capsular opacification is the main cause of the blurriness and it significantly interferes with daily life, laser treatment may be considered. The formal name is Nd:YAG laser posterior capsulotomy. It works by creating a small opening in the center of the cloudy membrane with a laser, reopening the pathway for light.
Because it is performed in an outpatient setting after numbing eye drops and typically takes a relatively short time, it is often described as a “simple procedure.” In practice, once the opening is made, the membrane does not grow back, so most people experience clearer vision after a single treatment. However, a short procedure time does not mean the patient’s eye condition can be treated lightly.
If a multifocal intraocular lens was implanted, even very subtle capsular changes can cause much more noticeable glare or halos. On the other hand, even if cloudiness is present, if it is mild, it may be better to monitor rather than rush into treatment. So, while many improve after one session, there are definitely cases where a cautious approach is needed depending on the type of intraocular lens and whether other eye diseases are present.
4. Why follow-up after laser matters: intraocular pressure, macula, and retina should be
checked together
Nd:YAG laser capsulotomy is an excellent treatment for posterior capsular opacification, but having the procedure does not mean eye care is “finished” afterward. According to a large French claims-data study (Dot et al., 2023), intraocular pressure elevation or macular edema has been reported in the early period after the procedure. Very rarely, the possibility of a retinal tear or retinal detachment should also be kept in mind.
Follow-up should be especially thorough for higher-risk groups with underlying conditions. People with diabetes should watch for macular edema (swelling of the macula) after the procedure, and those with high myopia or a long axial length should be evaluated for the risk of retinal traction due to vitreous changes inside the eye. People with elevated baseline intraocular pressure or glaucoma may also be more vulnerable to temporary pressure spikes after the procedure.
Even though the procedure does not touch the intraocular lens and instead opens the transparent membrane behind it to allow light through, it can still cause subtle changes that affect the “sensor” (macula) and “pressure” (intraocular pressure) inside the camera. Using prescribed eye drops as directed and checking retinal and pressure status at planned follow-up visits are key to protecting eye health.
✅Checklist to self-monitor before and after laser treatment
- Have you developed sudden, severe headaches or eye pain that is hard to tolerate?
- Have new flashes of light appeared at the edge of your vision, or become more frequent?
- Have floaters (speck-like shadows) suddenly increased a lot?
- Does part of your vision look like it’s being covered by a black curtain?
- Has your vision suddenly become much blurrier again, or started to look shaky?
If any of these apply, you should promptly visit an ophthalmology clinic to check the retina and intraocular pressure—even before your scheduled appointment.
5. Decision criteria to reduce the “recurrence” misunderstanding after surgery: monitoring
vs. YAG laser

Ultimately, a reasonable way to respond to posterior capsular opacification is neither to undergo a procedure automatically nor to endure symptoms without action. Even with the same diagnosis of posterior capsular opacification, the best management plan should be determined based on the severity of your symptoms and detailed exam findings.
If discomfort is mild or the main cause of blurriness is suspected to be another condition (dry eye, retinal disease, etc.), it may be necessary to confirm the cause first through regular ophthalmic exams rather than rushing into laser treatment. Conversely, if detailed testing shows that capsular clouding is the main culprit and visual quality in daily life has significantly declined, YAG laser can be an effective option.
| Category | Cases Where Observation is More Favorable | Cases Where YAG Laser May Be More Favorable |
|---|---|---|
| Level of Daily Discomfort | Blurring is mild and at a manageable/adaptable level | Blurring, glare, and light halos significantly disrupt daily life |
| Detailed Exam Results | Posterior capsular opacification (PCO) is mild, or checking for other retinal/IOP issues takes priority | Slit-lamp examination confirms PCO as the clear primary cause of vision loss |
| Treatment Direction | Avoiding unnecessary procedures and focusing on follow-up monitoring for other potential conditions | Opening the optical path via the procedure, while concurrently monitoring IOP, macula, and retina afterward |
6. Frequently asked questions (FAQ)
Q. My vision became blurry a few years after cataract surgery. Do I need to remove the lens and have repeat surgery?
Even if vision becomes blurry, it is uncommon to remove the implanted intraocular lens and perform repeat surgery. In many cases, the first step is to check for posterior capsular opacification, where the transparent membrane behind the lens becomes cloudy. If this is the cause, vision can often be restored by a simple outpatient laser procedure that leaves the
lens in place and opens only the cloudy membrane.
Q. Why does posterior capsular opacification happen, and how common is it?
It is a natural healing response that occurs when lens epithelial cells proliferate on the thin “bag” (posterior capsule) left inside the eye to hold the intraocular lens. It is a change that is not rare over time after surgery and is not a complication caused by a mistake in surgery. The timing and severity vary depending on an individual’s eye condition.
Q. What tests are done before YAG laser?
It is important to determine whether reduced vision is due to posterior capsular opacification or due to structural problems deeper inside the eye such as the macula, retina, or optic nerve. To do this, clinicians typically combine slit-lamp examination, fundus examination, visual acuity testing, and intraocular pressure measurement to judge whether laser treatment is appropriate.
Q. Can intraocular pressure rise after laser treatment? When should I come in to get it checked?
Temporary intraocular pressure elevation has been reported immediately after the procedure or within the first few days. In most cases it can be controlled with prescribed eye drops, but people with glaucoma or historically high intraocular pressure need extra caution. Following the schedule provided by your clinician to check intraocular pressure and retinal
status is the safest approach.
If your vision becomes cloudy again one day after cataract surgery, it’s easy to feel alarmed and think, “The surgery failed.” But you don’t have to stay stuck in that vague anxiety. The most important step is a detailed exam to determine whether the cause of the blurriness is posterior capsular opacification—and to decide on treatment only when symptoms and exam findings align.
Rather than forcing yourself to endure discomfort, consider getting evaluated to determine whether this is “frost on a window” or a problem inside the camera. With an accurate diagnosis and a tailored follow-up plan, you can maintain a bright, comfortable daily life without being thrown off by future changes in vision.
Sources
- Korea Disease Control and Prevention Agency (KDCA), National Health Information Portal: Health information on cataract/posterior capsular opacification, 2023
- Asan Medical Center, Guidance on Nd:YAG laser capsulotomy (condition and procedure information), year not specified
- Donachie et al., The Royal College of Ophthalmologists’ NOD cataract surgery: Report 9, *Eye*, 2023
※ The copyright for all content on this blog belongs to medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.
Recommended reads
