
Is sudden low back pain just a simple muscle strain, or could it be a herniated disc? This post covers a self-check checklist based on whether you have leg tingling/numbness, and explains why advanced imaging is not always needed right away. Learn the warning signs you should not ignore—such as toe weakness—and practical strategies to prevent recurrence.
“My back suddenly gave out and it hurts so much. Could it be a disc?”

Many people visit a clinic after “throwing out” their back while lifting something heavy or changing posture. Because the pain can be intense and unfamiliar, it’s natural to worry that it might be something serious. But you don’t necessarily need to panic. Even pain that makes it hard to breathe does not automatically mean a severe condition. If you know how to sort accompanying symptoms and warning signs first, it becomes much easier to manage that anxiety.
What clinicians check first is not simply how severe the pain is, but the direction the pain travels. It’s important to distinguish whether the pain stays around the low back, or whether it irritates nerves and radiates through the buttock and leg all the way to the foot.
1.Why “mechanical low back pain” is often suspected first after you “throw out” your back

When you’ve been sitting for a long time and stand up, your lower back can take a sudden load. A similar thing can happen in the split second you lift a heavy box. A large portion of acute low back pain that occurs this way falls under mechanical low back pain, such as a lumbar sprain.
Imagine your body as the electrical circuit system in a house. If you use too much power at once, the circuit breaker trips. The back works in a similar way: when the load exceeds what the ligaments can tolerate, nearby muscles contract strongly. It’s a defensive mechanism—like flipping the breaker.
When the muscles spasm and stiffen, you may feel pain that makes it hard to bend or straighten your back. But just as a dark house doesn’t mean all the wiring has been severed, severe pain alone does not prove that internal nerves have been seriously damaged.
If the soreness is localized around the low back, a lumbar sprain should be considered first. In these cases, symptoms tend to improve with rest and gradually easing the muscle spasm. Acute nonspecific low back pain often decreases within 4–6 weeks, although some people may have lingering symptoms and need ongoing management.
2. Key clues to distinguish simple muscle pain from a “disc (lumbar disc herniation)”

A “disc” that people commonly worry about—lumbar disc herniation (herniated intervertebral disc)—works differently from a lumbar sprain. If a lumbar sprain is a problem with the outer protective layer (muscles/ligaments), then a disc problem involves disc material between the vertebrae protruding and compressing a nerve. Specifically, the intervertebral disc is damaged and the inner nucleus pulposus pushes through the annulus fibrosus, leading to nerve compression.
Using the earlier analogy: it’s not just the breaker tripping—it’s more like the insulation on a wire inside the wall has been stripped. When a wire is damaged, the connected appliances start malfunctioning. When a spinal nerve is compressed, abnormal signals can be felt in the lower-body areas that nerve supplies.
That’s why the location of symptoms is a key criterion for differentiation. If your back simply throbs and hurts, that pattern is more commonly mechanical low back pain. On the other hand, if you feel tingling/numbness or an electric-like pain shooting down the leg, a disc-related lesion may be suspected. In real clinical practice, observing whether pain stays in the low back or travels down the leg is very helpful.
✅ Lumbar sprain vs. disc: symptom checkpoints
- The pain tends to stay only in the low back. (Suggests lumbar sprain)
- The pain radiates to the buttock/leg or includes tingling/numbness. (Suggests disc)
- Leg symptoms become more noticeable with coughing/sneezing/prolonged sitting.
- There is an area of reduced sensation (e.g., calf, top of the foot, sole).
- The ankle or toes feel weaker than before.
3. “Red flags” that require emergency care or prompt medical evaluation

Acute low back pain often improves gradually over time. However, not all pain should be brushed off. Under certain conditions, you need a careful medical evaluation. In medicine, these are called “red flags.”
If symptoms progress beyond tingling/numbness to actual weakness in the ankle or toes, you should be cautious. This may be evidence that a motor nerve is being compressed. Also, if sensation becomes dull in both legs or there are changes in bowel or bladder function, an emergency situation is more likely.
Beyond neurological abnormalities, a cautious approach is needed when systemic
symptoms are present. If there is unexplained weight loss or fever, an infectious condition should be considered. And if someone with a history of cancer develops new low back pain, prompt evaluation is also recommended.
[Is my low back pain an emergency? When you should seek care immediately vs. monitor symptoms]
| Category | Primary Symptoms and Management |
|---|---|
| When to seek immediate medical attention | Weakness in the ankle/toe muscles, bowel or bladder dysfunction, fever and chills, unexplained weight loss, new back pain in a patient with a history of cancer |
| When observation and monitoring are possible | Pain localized only to the muscles around the lower back, stiffness/aching after lifting heavy objects, absence of neurological abnormalities |
If red flags are present or symptoms are worsening, you should visit a medical facility without delay.
4. Does getting an MRI right away significantly help treatment?

When your back hurts and you go to the hospital, it’s easy to assume you need an MRI. The more anxious you feel, the more you want visual confirmation and reassurance. But in the early stage of acute low back pain, an MRI is not always recommended. MRI findings alone can’t definitively identify the cause of your current pain, and determining whether a finding is directly related to your symptoms requires correlating it with the history and physical examination.
In your 30s and 40s, degenerative changes are commonly seen as part of normal aging. If you get an MRI early when there is no leg tingling/numbness or red flags, you may incidentally discover degenerative findings that are unrelated to the current pain.
Because this can create unnecessary anxiety, it is better to perform an MRI when there is a clear possibility that it will change the treatment plan. A cautious and safe approach is to proceed with MRI when pain persists beyond a certain period despite initial conservative treatment, or when red flags are present.
5. Practical ways to break the cycle of “recurrence” after the pain settles
Severe low back pain often improves with appropriate rest and conservative management. It’s like turning the breaker back on and restoring normal power.
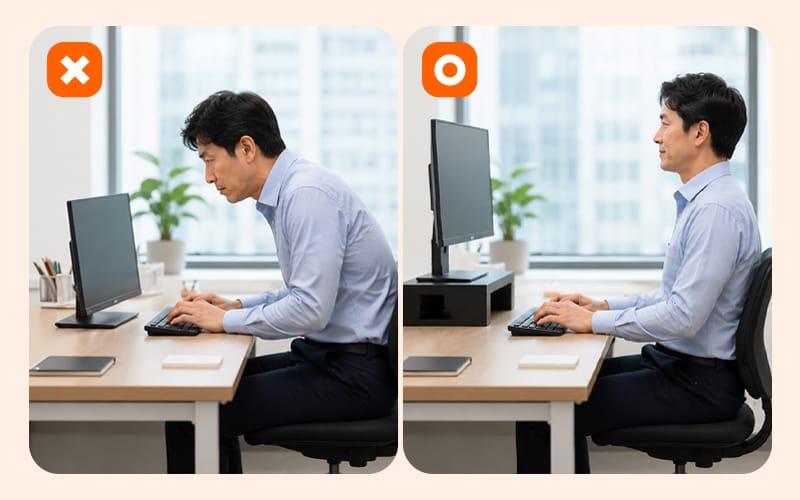
However, many office workers return to their old poor posture once the pain disappears. Sitting all day with your head pushed forward toward the monitor can make mechanical low back pain (including lumbar sprain) more likely to recur, so it’s important to make an effort to maintain good posture in daily life.
For the first few days right after you throw out your back, it’s best to avoid excessive movement. But once the pain becomes tolerable, starting light walking can help. If you lie down for too long, your core muscles weaken and recovery may actually slow down.
After the pain decreases, it’s important to review your workplace setup. Consider turning the small actions below into part of your work routine:
- After each meeting ends, walk in place for about 30 seconds
- Take work calls standing up instead of sitting
- Adjust your monitor to eye level to prevent looking down
These small movements can be even more effective for preventing recurrence than
treatment alone.
6. Frequently Asked Questions (FAQ)
Q. Can it still be a disc even if only my low back aches and throbs?
In the early stage of a disc problem, some people may have pain only in the low back. However, if there is no leg tingling/numbness or weakness at all and you mainly feel central low back stiffness, a lumbar sprain involving the muscles or ligaments around the spine is relatively more likely. It’s important to carefully monitor changes in accompanying symptoms.
Q. If I just lie down and rest for a few days, will I recover faster?
During the first 1–2 days when pain is severe, it’s good to rest and avoid overexertion. But if you continue lying down for a long time even after the pain settles, muscles can decondition and recovery may be delayed. Maintaining light activity within a tolerable range is generally more favorable.
Q. Why is it dangerous if I have a fever or the pain gets worse at night?
If pain worsens at night or you develop an elevated body temperature, it may not be simple muscle pain. This can be a red flag suggesting an infectious or inflammatory condition, so prompt medical evaluation is needed.
Q. When should I hurry to get medical care or consultation for acute low back pain?
If neurological symptoms appear—such as worsening tingling radiating down the leg or weakness when lifting the ankle or toes—seek care without delay. Consultation is also recommended when pain persists for more than 4–6 weeks without improvement.

To help you respond rationally to sudden low back pain, here are three decision criteria.
First, check the location: is the pain limited to the low back, or does it radiate down the leg?
Second, look for red flags that require urgent evaluation, such as leg weakness, bowel/bladder changes, or fever.
Third, if there are no red flags, prioritize conservative treatment and monitor progress rather than rushing into advanced testing.
Pain is a warning signal from the body, but with the right criteria and response, it can be managed and overcome. Rather than being overwhelmed by immediate anxiety, observe your body’s signals calmly and work toward returning to a healthy daily routine.
Sources
- Korea Disease Control and Prevention Agency (KDCA), National Health Information Portal: Low back pain / Herniated intervertebral disc (2023)
- Health Insurance Review & Assessment Service (HIRA), Coverage criteria for spine MRI
- Wallwork et al., The clinical course of acute, subacute and persistent low back pain, CMAJ (2024)
※ The copyright for all content on this blog belongs to medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.
Recommended reads
