
A child who frequently squints may not be doing it out of habit—it can be a sign of a vision issue. This post summarizes structural warning signs that warrant an eye exam, along with a checklist parents can use at home.
“My child keeps squinting—could their eyesight be getting worse?”

Many parents come to the clinic with this concern. Some even blame themselves, wondering if early screen exposure caused it. But noticing this structural signal—something that can appear as a child’s visual system changes—and deciding to check it now is already a strong first step.
If you delay a hospital visit after hearing comments like, “They’ll grow out of it,” it may become harder to correct the child’s vision later.
In pediatric ophthalmology, when we see a child who squints, the first step is to confirm one key point: is it simply a habit, or a compensatory behavior due to reduced vision?
1. Why can children squint to “see better”?
When a child unconsciously narrows their eyes to see more clearly, it may be a
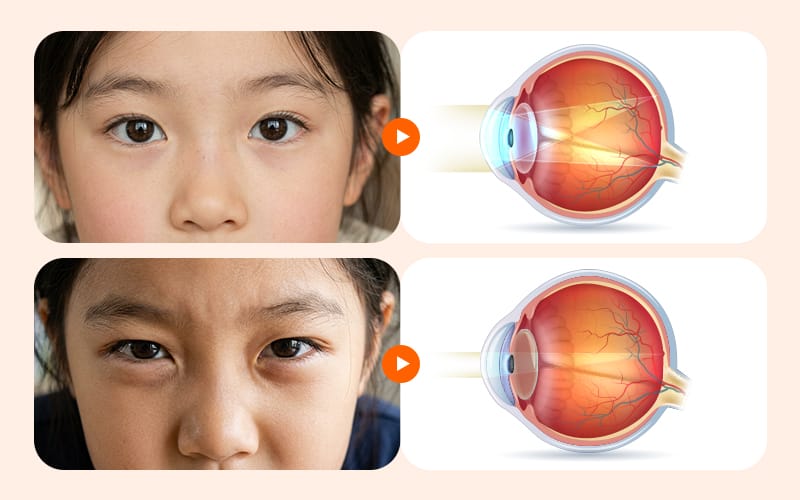
“compensatory behavior.” It’s easiest to understand by thinking of a camera aperture. When you narrow the aperture, the pathway for light becomes smaller, and focus tends to look clearer across distances. A similar effect can occur in the human eye.
Medically, this is called the “pinhole effect.” When a refractive error (such as myopia or astigmatism) causes the retinal image to become blurry, a child instinctively narrows their eyelids. Squinting reduces scattered light, which can temporarily make objects look sharper.
In other words, the child is not intentionally developing a bad habit. They may be unconsciously “stopping down the aperture” to see the board or TV a little better. However, squinting alone cannot confirm the cause. It can also appear alongside risks such as strabismus or amblyopia, so it’s best to identify the exact cause through an eye exam.
2. Why you shouldn’t delay glasses and testing in early elementary school

Unlike adults, a child’s vision is not fully developed at birth—it gradually matures with growth. In particular, around ages 7–8 is a sensitive period for visual development. Using a camera analogy, it’s like the lens and sensor are interacting to set the optimal image quality.
If significant refractive error or a difference in vision between the two eyes occurs during this period and appropriate glasses are not prescribed, the brain continues receiving only blurry images. If evaluation and treatment are delayed, even after glasses are provided later, corrected vision may not improve enough and can become fixed as “amblyopia,” lowering expectations for recovery.
The idea that wearing glasses at a young age makes eyesight worse is a misconception. Glasses are an essential tool when refractive error is significant or when there is a large difference between the two eyes, because they help form a clear image on the retina and support normal development of visual function. To protect this sensitive developmental window, timely evaluation in the early elementary years is important.
✅ When it’s a good idea to move up the exam appointment (Sensitive-period checklist)
- Over the past month, you’ve frequently noticed your child narrowing their eyes when looking at the board or TV.
- A school screening or infant/toddler health check found a difference in visual acuity between the two eyes.
- When focusing on objects, your child repeatedly tilts their head to one side or closes one eye.
3. 근시일까 사시일까? 집에서 확인하는 징후 비교

What caregivers most want to know is: “Is it myopia, astigmatism, or strabismus?” Squinting is often linked to refractive error, but it’s difficult to conclude based on a single behavior. If you only think about refractive error, you may miss hidden strabismus or amblyopia. By looking at behavior patterns at home, you can roughly gauge what direction of testing may be needed.
| Signs Observed at Home | Suspected Conditions & Next Steps (Tracking/Testing) |
|---|---|
| Squinting or moving closer when looking at a distant blackboard or TV | May be associated with refractive errors (myopia/astigmatism); tracking the frequency and getting a refractive test is recommended |
| Closing one eye due to glare under bright outdoor sunlight on a clear day | Suspected strabismus spectrum (e.g., intermittent exotropia); consider a detailed examination including a strabismus evaluation |
| Experiencing misaligned eye focus when tired or spacing out | Strabismus and amblyopia evaluation is essential if accompanied by closing one eye or ocular misalignment |
| Becoming noticeably uncomfortable or irritated when one eye is covered | Detailed evaluation of binocular visual acuity to check for differences in vision between both eyes (anisometropia) |
Keeping detailed notes of what you observe at home can be very helpful during the visit. However, these behaviors alone cannot be used to self-diagnose a specific condition, so getting a specialist’s differential diagnosis is the safest approach.
4. Treatment to slow vision decline: when and how should it start?

If testing confirms a refractive error, an appropriate management strategy is planned based on the child’s situation. If progression is not rapid, the foundation is wearing glasses with an accurate prescription and tracking vision regularly.
However, the approach may differ if myopia is progressing faster than peers or if there is a family history of high myopia. In such cases, more active interventions to slow progression can be considered. Options include low-dose atropine eye drops, specially designed functional spectacle lenses, and corneal reshaping lenses (dream lenses).
Many studies have reported that these options may help suppress abnormal elongation of the eyeball. Still, because methods vary and each has pros and cons, treatment decisions should be made in consultation with medical professionals. Even with treatment, regular follow-ups are important to monitor whether myopia-control effects are sufficient.
5. Why outdoor activity may help—along with limiting smartphone use

At home, the biggest focus for vision care is often screen time. Multiple studies have shown that excessive near work and screen exposure are associated with myopia progression. For environmental management, realistic time adjustment tends to be more important than attempting complete avoidance.
In addition, increasing outdoor time—alongside reducing near work—can be a relatively safe and useful pillar of management. Outdoors, the eyes shift focus from a fixed, close distance in a small room to farther distances in a wider environment. It’s like switching a camera that’s been stuck in macro mode into landscape mode, reducing strain on the lens.
Rather than forcing a strict schedule, consistent habits—like walking around the playground after school or taking a weekend park walk—may help relieve fatigue in a child’s focusing system.
6. Frequently asked questions (FAQ)
Q. My child only squints once in a while when looking at the board. Do we still need an eye exam?
If squinting appears only at certain distances (like the board), it may be an early sign of refractive error (myopia or astigmatism). Many children don’t recognize gradual vision decline themselves, so if this compensatory behavior repeats, it’s a good idea to confirm the exact status through a refraction test.
Q. At the school vision screening, there’s about a one-line difference between the two eyes. Is that okay?
You should consider the possibility of anisometropia (a meaningful difference between the two eyes). More important than the one-line difference itself is whether development is delayed compared with peers and whether the weaker eye is at risk of progressing to amblyopia due to the imbalance. A comprehensive ophthalmic exam is the safer choice.
Q. Can anyone use atropine eye drops to slow myopia progression?
Low-dose atropine may help slow myopia progression, but it is not applied uniformly to every child. Side effects such as light sensitivity or discomfort during near work have been reported depending on the child, so it should only be used with an ophthalmologist’s prescription and regular follow-up.
Q. If we visit the eye clinic after symptoms appear, what tests will be done?
Depending on the child’s eye condition, basic visual acuity testing and refraction testing are performed. Cycloplegic refraction may be needed to detect hidden hyperopia or determine an accurate myopia prescription. Evaluation for strabismus and binocular vision may also be included. For accurate diagnosis, bringing a video showing the child squinting in daily life can be helpful.

Here are three key standards to remember to protect your child’s visual health.
First, a child’s squinting may be less of a simple habit and more of a signal of refractive error, strabismus, or amblyopia—an attempt to make a blurry world look clearer.
Second, it’s important to differentiate risk factors in the early school-age period around 7–8 years old. If this window is missed, expectations for later correction and recovery may be lower.
Third, lifestyle management—such as wearing glasses, myopia-control treatment, and outdoor activity—should be designed with medical professionals based on the child’s individual condition.
Even if you’re worried about your child’s eyes right now, it may not be too late. If you notice small behavioral changes and confirm the cause through testing, there are still meaningful ways to support healthy visual development.
Sources
- Journal of the Korean Ophthalmological Society. Clinical characteristics of functional (psychogenic) visual loss in children. (2016)
- Korean J Ophthalmol. Korean Intermittent Exotropia Multicenter Study Questionnaire. (2024)
- JAMA. Vision in children ages 6 months to 5 years: Screening (USPSTF). (2017)
※ The copyright for all content on this blog belongs to medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.
Recommended reads
