
This post explains the difference between AC joint pain—where a single pinpoint at the very top of the shoulder near the end of the collarbone hurts—and rotator cuff tears. It also outlines how to differentiate distal clavicle osteolysis (DCO) in a fitness-focused person in their 40s, along with step-by-step treatment criteria.

When someone comes in with shoulder pain, there are two things clinicians check first: the exact location of the pain and which movements make it worse. In particular, if a single pinpoint at the very top of the shoulder hurts, AC joint pain becomes a leading consideration. This can be an important clue suggesting accumulated fatigue and stress within the joint structure rather than a simple muscle strain.
“My shoulder hurts like it’s being poked right where my bra strap sits.” This is a common complaint among people in their 40s who enjoy weight training. Many patients visit with the same concern. If it doesn’t improve even after resting for over a month, it’s easy to feel frustrated—and some even blame themselves for “overdoing it.”
This kind of localized pain is often less consistent with a straightforward muscle tear. It may be caused by repeated mechanical friction concentrated in a very small joint area. That’s why a careful, step-by-step process of differentiating possible conditions is needed.
1. How is “one pinpoint” pain at the top of the shoulder different from a rotator cuff injury?
When shoulder pain begins, many people first suspect a rotator cuff tear. However, rotator cuff conditions tend to present differently when you lift your arm. The pain often spreads more broadly across the shoulder or down into the upper arm. By contrast, if you can point with a single finger to the exact end of the collarbone at the very top of the shoulder, that pattern suggests something else.
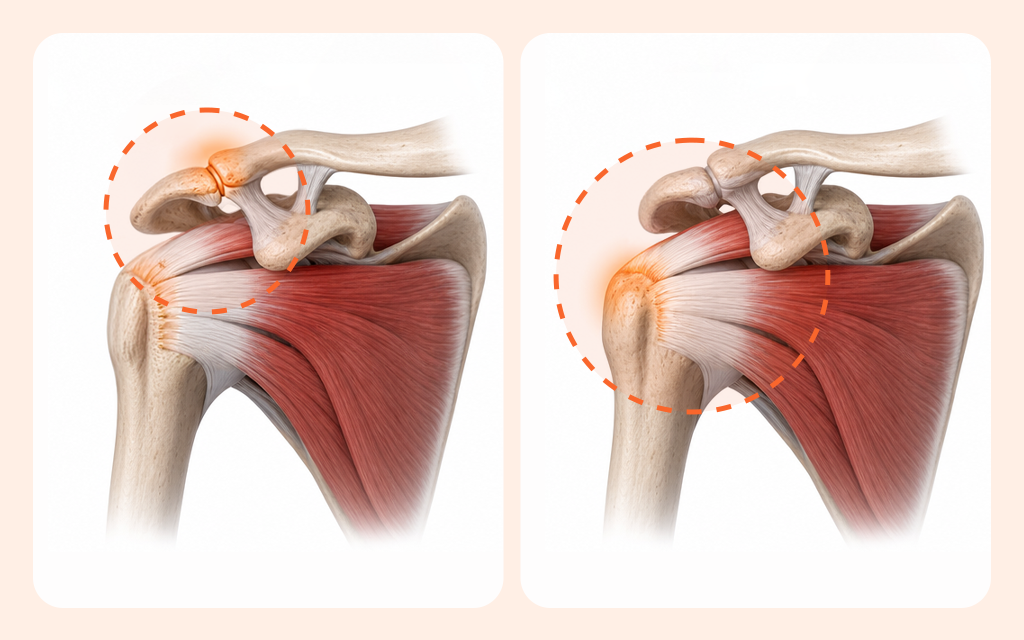
This type of localized tenderness points toward a lesion of the acromioclavicular (AC) joint. The AC joint is a small joint where the acromion (the highest point of the shoulder blade) meets the end of the clavicle. To make it easier to visualize, think of a rope and a hinge. If the rotator cuff is like a “rope” that pulls and moves heavy loads, the AC joint is like a small “hinge” that stabilizes the bony framework so it doesn’t wobble. A problem where the rope frays and a problem where the hinge becomes stiff can feel very different.
This small hinge-like joint may look like it barely moves, but it subtly rotates when you raise your arm or bring it across your body. It also has to tolerate substantial pressure during those motions. If the pain is concentrated in one pinpoint location, it’s reasonable to suspect fatigue or irritation in that hinge structure.
2. Pain that worsens after bench press—could distal clavicle osteolysis be the cause?

Among people in their 40s who do weight training, AC joint pain is fairly common.
Movements that press and bring the arms inward toward the chest—such as bench press, chest fly, and push-ups—can contribute. These loads can create ongoing mechanical friction at the “hinge” area near the end of the clavicle.
When these movements are repeated, overuse-related irritation can accumulate in the AC joint. In some individuals, imaging may even show bone-resorptive changes such as distal clavicle osteolysis (DCO). Rather than failing all at once, it can resemble a hinge gradually developing tiny looseness and then feeling stiff at certain angles. Because pain at the top of the shoulder can overlap with rotator cuff problems, impingement syndrome, or even cervical spine issues, careful differentiation is important.
If it’s simply post-workout muscle tightness, rest typically leads to improvement. But if joint friction is the driver, sharp pain tends to reproduce with specific movements. A common maneuver is the “cross-body adduction test,” which checks whether pain occurs when you bring the arm across the chest. If this produces a deep ache or sharp discomfort, AC joint compression can be suspected.
✅Workout log checklist (finding clues from pain)
- Do you clearly recognize the specific exercise that triggered the pain (bench press, fly, etc.)?
- In the past 2–4 weeks, did you increase the weight or range of motion beyond your usual level?
- When you bring your arm across your chest, does a stabbing pain reproduce?
3. If arthritis is seen on MRI, is it always the cause of the pain?

Many people visit a clinic for shoulder pain and undergo imaging. They are often surprised to hear that the AC joint shows “degenerative arthritis.” However, changes seen on imaging are not automatically the cause of the current pain.
After the 40s, degenerative changes are commonly observed even in people who don’t heavily use their shoulders. Research has also found these findings routinely in asymptomatic patients who had shoulder MRIs. It’s like seeing a bit of rust on a hinge of an old door—something that can be common.
That trace does not necessarily prove the door is broken. So, clinicians typically do not plan aggressive treatment based on imaging alone. The pain location the patient indicates, the findings reproduced during physical examination, and the imaging results should align. When all three point in the same direction, the finding is interpreted as clinically meaningful.
4. Persistent pain: when is conservative care vs injection therapy more favorable?

For non-traumatic pain, the first-line approach is conservative care. This typically includes modifying training, taking anti-inflammatory medication, and resting. It’s similar to not replacing a door immediately just because the hinge squeaks—first you lubricate it and tighten the screws.
If pain occurs only with certain movements, it’s often best to adjust the range of motion and rest. On the other hand, if pain is severe even at rest and disrupts sleep, the next step may be considered. In such cases, an ultrasound-guided injection can be discussed for short-term pain control and to help confirm the pain source and lesion localization.
An ultrasound-guided injection delivers medication into the narrow joint space to reduce inflammation. However, it can be difficult for a single injection to make the pain disappear completely, because it does not fundamentally eliminate the physical friction between bone and cartilage. It is safer to view injection therapy as a tool for short-term symptom relief and diagnostic support.
✅Pre-visit consultation checklist (setting the treatment direction)
- During chest exercises, at which angle does the stabbing pain most often occur?
- Is the whole shoulder painful, or can you clearly pinpoint one spot at the end of the clavicle?
- Even after avoiding the triggering exercises, do you still feel discomfort when sleeping or getting dressed?
5. If it still hurts despite adequate rest, when should surgical treatment be considered?

Even after months of training modification and conservative care, functional limitation may remain significant. If the painful area is relatively well localized, surgery may be considered after careful discussion with a clinician. A commonly performed procedure for AC joint conditions is arthroscopic distal clavicle resection.
This works by increasing the space between the contacting bones to reduce physical friction. It’s like smoothing the worn end of a hinge to create enough clearance for smoother movement again. In selected patients, improvements in pain and functional measures may be expected after surgery, but consistent rehabilitation should accompany recovery.
If the situation is an “AC joint separation (dislocation)” caused by an external impact such as a fall, the approach differs. In that setting, treatment varies according to the Rockwood classification, which grades injury severity. When high-grade instability is present, fixation and reconstruction surgery may be actively considered. For borderline intermediate grades such as type III, decisions are individualized by weighing instability and the patient’s daily activity demands.
6.Frequently Asked Questions (FAQ)
Q. The very top of my shoulder hurts when I press on it—what test is done first?
In the clinic, the first step is to assess whether there was trauma. Then, a careful physical exam is performed to check localized tenderness and pain-provoking movements. A basic X-ray is commonly done first to evaluate bony alignment, with ultrasound or MRI added if needed.
Q. When can I return to bench press, and how should I modify it?
During the acute pain phase, it is generally recommended to stop pressing movements or cross-body adduction motions that irritate the joint. After symptoms settle, restart cautiously by significantly reducing the weight and limiting the range of motion. If it continues to overload the area, the training method should be changed.
Q. If X-ray or MRI shows AC joint arthritis, does it always require treatment?
Even if imaging shows arthritic changes, focused treatment may not be urgently needed if it does not match your current symptoms. After the 40s, degenerative findings are commonly seen even in people without shoulder pain.
Q. At what point should I consult a clinic?
If a stabbing, pinpoint pain persists for more than a week despite resting from exercise. Or, if sharp discomfort continues during daily activities such as bringing the arm across the chest, evaluation is recommended to differentiate the cause.

When facing shoulder pain, it’s easy to assume it must be a broad muscle problem—or to rely only on imaging results. But the key to assessing AC joint pain is accurately identifying the pain location and checking which movements reproduce it.
You don’t necessarily need to carry the heavy worry that you “seriously damaged the joint” just because you trained incorrectly. Based on objective diagnostic criteria and a record of pain-provoking exercises, I hope you can work toward the safest and most appropriate treatment plan for your current situation.
Sources
- Clinics in Shoulder and Elbow, Mid- to long-term success rate and functional outcomes of acromioclavicular injections in patients with acromioclavicular osteoarthritis, 2023
- Clinics in Shoulder and Elbow, Diagnostic value of a preoperative acromioclavicular injection for symptomatic acromioclavicular osteoarthritis, 2024
- Orthopaedics & Traumatology: Surgery & Research, MRI findings of acromioclavicular joint osteoarthritis are the norm after age 40, 2023
※ The copyright for all content on this blog belongs to medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.
Recommended reads
