
This post lays out practical criteria for deciding when to choose higher-cost advanced imaging in shoulder pain treatment. You’ll see how a step-by-step approach to testing can help set an efficient treatment direction.
“My shoulder keeps hurting—should I get an MRI first to know the exact cause?”
It’s completely understandable to hesitate because of the cost. People whose shoulders rarely get a break due to work and household responsibilities often worry that if they don’t get an expensive test, they might miss something serious.
However, when clinicians first meet a patient with shoulder pain, the very first thing they check is not “which advanced imaging machine should we use?” A physical exam comes first to assess how limited the shoulder function is right now.
In the clinic, the priority of tests is usually decided based on the exam and a basic X-ray. Jumping straight to high-cost imaging may not be the most efficient approach.
Through this article, I hope you can confirm an appropriate testing sequence and clear decision criteria that fit your situation.
1. Shoulder pain diagnosis: why do the exam and X-ray come first?
Finding the cause of shoulder pain is similar to a building safety inspection. A simple X-ray is like a basic check of the building’s steel framework. A shoulder MRI, on the other hand, is more like a detailed blueprint that inspects internal piping and insulation for a full-scale repair plan. If you don’t yet know whether the issue is in the framework or the outer wall, there’s no reason to start by ordering an expensive blueprint. Many people mistakenly believe that X-rays “only show bones,” so they assume X-rays are meaningless for tendon-related pain.
But in real clinical practice, X-rays provide very important clues. Beyond checking for fractures or dislocations, they can also help identify bone spurs (osteophytes) or calcifications that may irritate tendons. Some studies have reported that certain bony changes on X-ray can be observed alongside rotator cuff problems. An X-ray alone cannot confirm a tear, but it becomes a key hint for deciding what the next test should be.
If it’s mild muscle soreness or early-stage changes, a physical exam and basic X-ray may be sufficient to establish a conservative treatment plan. Only when a significant structural problem is strongly suspected is it appropriate to proceed to the next level of advanced imaging.
2. Shoulder ultrasound vs. MRI: what should you choose?

After basic testing, if soft tissues such as the rotator cuff tendons or the bursa need to be evaluated, the options begin to diverge. Ultrasound is like tracing along a building’s outer wall and checking for cracks in real time. A major advantage is that it allows dynamic observation—moving the joint during the exam to see where impingement occurs. When performed by an experienced clinician, ultrasound can show specificity close to that of MRI (around 90%), making it cost-efficient as well.
A shoulder MRI, in contrast, provides a three-dimensional view of the overall structure. It can assess not only the degree of tendon damage but also whether surrounding muscles have lost function and undergone degeneration. That’s why it’s important to make a reasonable choice by weighing symptoms and financial burden together.
[Shoulder ultrasound vs. MRI: comparison of pros/cons and key features by test type]
| Method | Key Advantages & Scope | Limitations & Considerations |
|---|---|---|
| Shoulder Ultrasound | Relatively lower financial burden; advantageous for identifying dynamic impingement and the presence of primary tears | Highly dependent on the examiner's proficiency; limited in identifying deep lesions or complex issues hidden by bone |
| Shoulder MRI | Comprehensive evaluation of soft tissue structures, assessment of muscle fatty degeneration, and precise surgical planning | Higher financial burden (potential out-of-pocket expenses); integrated interpretation with clinical findings is essential for certain lesions |
If you want to reduce cost while first checking whether a tear is present, ultrasound can be a practical alternative. If the situation is complex enough to discuss surgery, or if the entire internal structure of the joint needs careful evaluation, the informational value of MRI becomes much greater.
✅Key checkpoints when choosing ultrasound vs. MRI
- Is ultrasound’s real-time dynamic assessment advantageous for confirming my current symptoms?
- What is the examiner’s level of musculoskeletal expertise, and how comprehensive is the scan?
- Is this a situation where surgical treatment is being considered, requiring a full assessment of soft tissue status?
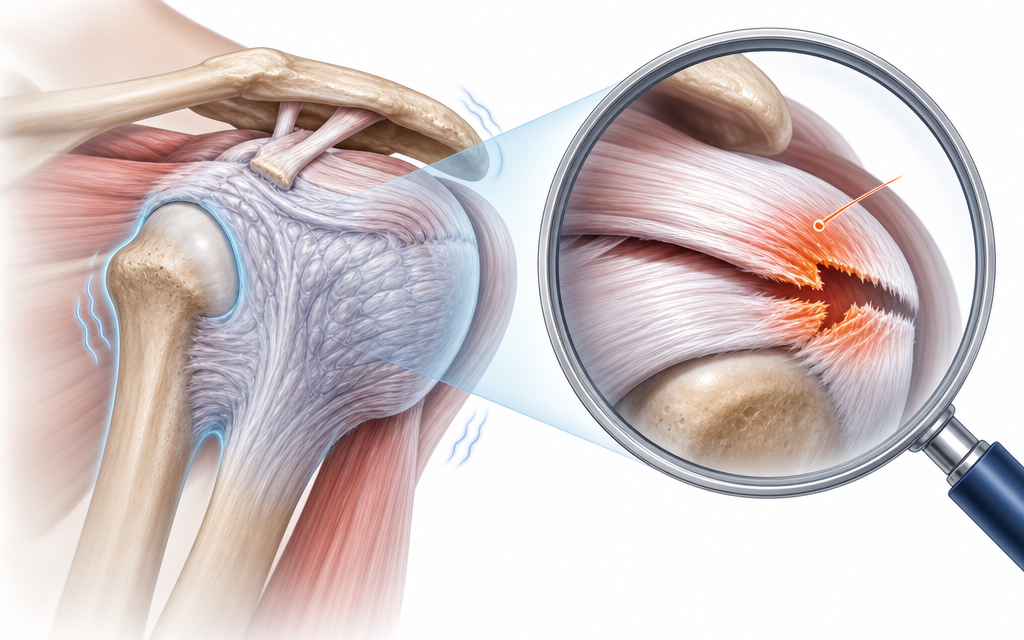
3. Why treatment isn’t decided immediately even if an MRI shows a “tear”

When you receive an imaging report, you may see the word “tear.” Many people then feel intense anxiety, thinking they need surgery right away. But just because an old building blueprint shows worn piping or small cracks doesn’t mean the building is about to collapse. Medically, it’s difficult to conclude that an abnormal imaging finding is the sole cause of the pain you’re currently experiencing.
In fact, multiple literature reviews involving asymptomatic adults have commonly reported cases where MRI abnormalities are found despite no pain at all. That doesn’t mean MRI results are meaningless. Imaging is not a tool that determines the cause and provides a single “correct answer” on its own—it’s highly valuable information that helps narrow down treatment options.
Treatment direction is determined by comparing pain severity, the degree of limitation in lifting the arm, and physical exam findings together. Even if imaging shows abnormalities, if daily use is possible and the patient responds well to conservative treatment, continuing rehabilitation may be a reasonable approach. On the other hand, if there is significant loss of strength, surgical treatment can be discussed more actively.
4. If cost is a concern, how can you set a reasonable testing priority?

The greater the financial burden, the more you need a clear standard. The recommended criterion is just one: “Will this test change my treatment plan?” Under Korea’s National Health Insurance system, a shoulder MRI may be classified as non-covered (out-of-pocket) if specific indications or allowed frequency criteria are not met. Insisting on advanced imaging from the start can increase the burden without improving decision-making.
Testing priority can be categorized by clinical situation as follows:
- Sudden pain and loss of function after trauma: ruling out fracture or dislocation is urgent, so a plain X-ray is the top priority.
- Suspected rotator cuff tear but cost is a concern: an ultrasound performed by a skilled examiner can be an excellent first-line screening tool.
- No improvement despite conservative care and surgery is being discussed: because associated lesions and muscle condition must be assessed accurately, a shoulder MRI has high value.
With this approach, testing costs shift from a blind “reassurance expense” to a rational “decision-making expense” that clarifies the next step. If it’s not an acute trauma situation, starting with an exam and X-ray and monitoring progress is a safe, cost-efficient approach.
✅Questions that can be helpful to confirm during a clinic visit
- Based on the exam and basic X-ray alone, is it possible to estimate the primary cause at this stage?
- Is this the point where advanced imaging is necessary to change the treatment plan (e.g., injection or surgery)?
- Is it likely that my symptoms meet the insurance coverage criteria for an MRI?
5. When it may be worth considering additional tests even if it looks like frozen shoulder
Frozen shoulder (adhesive capsulitis) is a condition in which inflammation develops in the joint capsule surrounding the shoulder, causing the entire joint to become stiff. People often feel reassured after being told they have frozen shoulder, thinking, “So it’s not a tendon tear.” However, it’s not uncommon for rotator cuff damage to be hidden inside a globally stiff joint—like damage concealed behind a building’s insulation.
The hallmark of frozen shoulder is severe limitation in range of motion both when you lift your arm yourself and when someone else tries to lift it for you. But sometimes, even when the shoulder seems globally stiff, a distinctive pattern appears where the arm can still be raised to some extent in a specific direction (e.g., forward elevation). According to research, this pattern may be associated with a higher likelihood of a concurrent rotator cuff tear.
If the main feature is simply a clear, overall restriction of movement, it’s best to focus on conservative treatment targeting frozen shoulder. If, however, range of motion is unusually preserved in a particular movement or noticeable weakness is observed, it can be safer—based on the clinician’s judgment—to further differentiate associated lesions using ultrasound or MRI.
6. Frequently Asked Questions (FAQ)
Q. Can an ultrasound alone confirm a rotator cuff tear?
According to studies, ultrasound performed by an experienced examiner can show diagnostic performance similar to MRI for rotator cuff tears. However, ultrasound has limitations because it depends heavily on the equipment and the examiner’s skill. It may be limited in evaluating deep structures or complex lesions obscured by bone, so supplementation may be needed depending on physical exam findings.
Q. In what situations can a shoulder MRI be non-covered (out-of-pocket)?
Under Korea’s National Health Insurance criteria, if you do not meet coverage requirements—such as specific suspected conditions (indications) or allowed frequency—an MRI may be applied as non-covered. If cost is a concern, it’s practical to discuss step-by-step with your clinician whether your current condition is likely to qualify for coverage, or whether ultrasound can serve as a first-line alternative.
Q. If an MRI shows a tear but my pain isn’t severe, can I delay treatment?
The severity of imaging findings and the pain or functional loss you actually feel do not always match. If you can use your arm in daily life and pain is well controlled, it may be reasonable to discuss with your clinician and consider rehabilitation-focused conservative treatment first, rather than deciding on surgery based only on the report.
Q. Before deciding on surgery, what should be checked on MRI?
For shoulder MRI, beyond evaluating the rotator cuff tendons, it can be highly specific for distinguishing deep internal findings such as SLAP lesions or Bankart lesions. These details provide an important basis for judging whether surgical repair is feasible and for estimating recovery potential after surgery.

In shoulder pain treatment, advanced imaging is not a magical tool that finds every hidden condition perfectly. It is a decision-making aid that helps guide you toward safer and more effective treatment. Using the physical exam and X-ray as the framework, and then choosing ultrasound or shoulder MRI step-by-step based on your symptoms and situation, is the most reasonable approach.
You don’t have to hold onto vague anxiety that your condition will worsen if you don’t get an expensive test right away. Simply communicating in detail with your clinician—how limited your shoulder function is and which movements are most uncomfortable—can be enough to fasten the first button correctly for proper treatment.
Sources
- Ministry of Health and Welfare (Korea) and Health Insurance Review & Assessment Service (HIRA). Coverage criteria for magnetic resonance imaging (MRI). (Refer to the most recent official notice.)
- Chae-won Kang · Hyo-young Lee. A Korean study comparing ultrasound and MRI in diagnosing rotator cuff tears (2022).
- Farooqi et al. Diagnostic accuracy of ultrasonography for rotator cuff tears: A systematic review and meta-analysis(2021).
※ The copyright for all content on this blog belongs to medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.
Recommended reads
