
When choosing a thyroid clinic, what matters more than advertising is the risk category of your nodule. Use the K-TIRADS question framework, understand criteria for active surveillance, and learn the respective roles of endocrinology and surgery so you can prepare for your visit without regret.
“I don’t know what to ask during such a short appointment.”

Many people leave consultations feeling disappointed because they didn’t know what to talk about. That usually happens when you don’t have a “map” of your current condition. If you don’t know whether you’re still at the “screening” stage or already at the “diagnostic” stage—and if you don’t know your risk score—you can’t ask the right questions.
To reduce vague fear, set just three criteria before your visit: your risk category (a number), the treatment direction (observation vs surgery), and a long-term follow-up system. With these in place, you can make a decision you won’t regret—no matter which hospital you go to.
1. Thyroid evaluation: the difference between a “satellite map” and an “on-site
investigation”

Thyroid testing is like reading a map. An ultrasound is a “satellite map (screening test)”—like looking down at a forest from above. You can tell whether there’s a lump and what the terrain looks like, but it’s hard to know exactly what’s inside. By contrast, a fine-needle aspiration (FNA) or biopsy is an “on-site investigation (diagnostic test)”—like digging into the ground directly.
Many people receive a thyroid ultrasound as part of a health checkup “package.” However, the overall direction of recommendations—such as those from the USPSTF (U.S. Preventive Services Task Force) and Korean guidance—has been not to recommend routine screening ultrasounds for asymptomatic adults. The goal is to reduce unnecessary treatment driven by overdiagnosis. In other words, it’s to avoid mistaking a rock’s shadow for a predator because you keep checking the satellite map too often.
But if you feel a foreign-body sensation in your throat, can feel a lump, or notice voice changes, the situation is different. In that case, evaluation for diagnostic purposes—not screening—is essential. When choosing a clinic, it’s more important to confirm whether they first assess your symptoms and risk factors (family history, radiation exposure, etc.) and move to advanced testing (the “on-site investigation”) only when needed, rather than offering a “one-and-done checkup” approach.
2. Nodule grading: ask “What’s my score?” rather than “Is it cancer?”
In the exam room, asking only “Is it cancer or not?” is like asking whether the weather is “good.” Clinicians communicate in probabilities—like “a 70% chance of rain.” To make your visit more efficient, ask for your nodule’s grade (number).
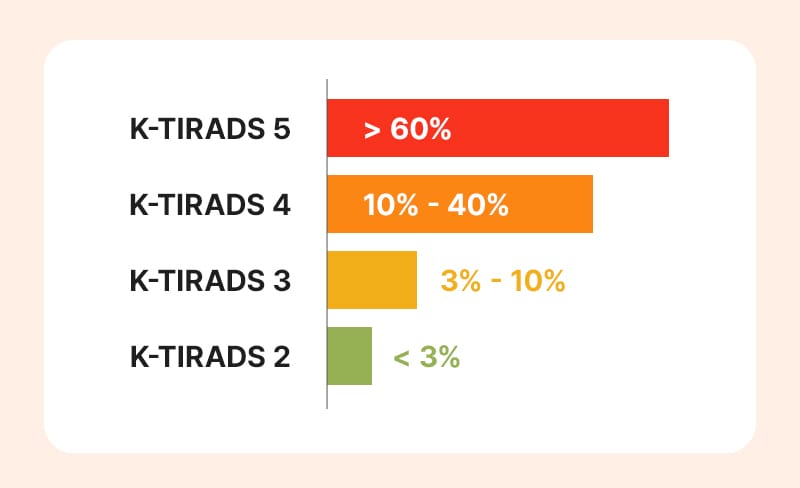
In Korea, K-TIRADS (Korean Thyroid Imaging Reporting and Data System) is commonly used. It assigns a category based on ultrasound features such as shape, margins, and echogenicity; a higher category generally indicates a higher risk of malignancy.
If you had an FNA, results are categorized using the Bethesda System. If you leave with only “It looks okay, let’s watch it,” you may feel anxious again at home. Instead, ask: “Does my nodule fall into the K-TIRADS high-suspicion category?” You’ll get a clearer, evidence-based explanation. If you obtain this grade in writing, continuity of care is easier even if you change hospitals later.
✅ Grade-check checklist
- What is my nodule’s K-TIRADS (ultrasound) category/score (or stage)?
- (If FNA was done) What Bethesda category is it?
- At this grade, what approximate probability of malignancy do you estimate?
- Can I receive copies of the report and the imaging files (CD)?
3. Endocrinology vs surgery: who should “hold the map”?

A thyroid treatment journey often involves two specialists: a “navigator (endocrinology)” who plans the overall route and monitors the “weather” (hormones), and a “helmsman (surgery)” who takes control when a physical removal is needed. Depending on your “map,” the lead physician may differ.
In general, endocrinology leads care for thyroid function issues (hyperthyroidism/hypothyroidism), nodule surveillance, and long-term management after surgery. On the other hand, once cancer is diagnosed and surgical removal is decided, the role of a thyroid endocrine surgeon (or an ENT surgeon, depending on the system) becomes critical.
When choosing a hospital, check whether there is a collaborative (multidisciplinary) system between these roles. If surgery is not urgent, a thorough diagnostic and follow-up system in endocrinology matters. If surgery is unavoidable, evaluate the surgeon’s experience and whether post-operative management (voice/vocal cord issues, calcium levels, etc.) is well organized. Especially if you were told “this nodule is borderline/uncertain,” a system where
multiple departments discuss the case can provide a safer “map” than a single opinion.
4. Surgery vs watchful waiting: where is the decision point? (Active surveillance)
For thyroid cancer—especially low-risk papillary microcarcinoma—“active surveillance” is increasingly recognized as a treatment option instead of automatic surgery. This is not neglect. It means “keeping the radar on under strict monitoring.” It’s like watching closely rather than evacuating if the route remains safe even when a storm is nearby.
The decision point depends on conditions. If the tumor is near the trachea or the recurrent laryngeal nerve (vocal cord nerve), or if lymph node metastasis is suspected, surgery may be considered without delay even if the tumor is small. If the location is considered safe and reliable follow-up is feasible, active surveillance can be discussed.
For people living overseas, “ability to follow up” becomes a key variable. Consider whether you can obtain ultrasounds using a comparable protocol after returning, and whether visits every 6–12 months are realistic. Even if observation is medically feasible, if anxiety is severe or clinic visits are difficult, surgery may be the more practical and reassuring option.
✅ Checklist for deciding treatment direction
- Does my tumor’s current location/status fall into the “active surveillance” candidate group?
- What specific criteria would trigger switching from surveillance to surgery (size change, lymph nodes, etc.)?
- Because I live overseas / far away, regular follow-up is difficult—what approach do you recommend in this case?
5. Treatment is not the end: confirm the “long-term management” system

Thyroid treatment does not end with surgery. It is a long-term journey to balance hormones and reduce recurrence risk. So when choosing a hospital, evaluate not only “surgical skill,” but also whether there is a system you can stay with over time.
Post-operative issues such as hypoparathyroidism (hypocalcemia) or voice changes can significantly affect daily life. Even at a large hospital, if communication is difficult or urgent responses are slow, anxiety increases. Check whether you can get prompt advice if complications occur and whether there is an emergency contact system for nights/weekends.
If you may move or transfer care, “data compatibility” is also important. Your medical records (your “map”) should connect smoothly when you switch hospitals. At the end of visits, build the habit of collecting the following materials.
✅Essential documents to prepare for transfer of care or returning home:
- Original thyroid ultrasound/CT imaging files (CD/USB)
- Biopsy slides and pathology reports (English/Korean)
- Operative report (including procedure name and detailed extent of resection)
- Most recent blood test results (to track hormone trends)
6.Frequently Asked Questions (FAQ)
Q. How can I check my K-TIRADS or Bethesda category?
Ask your clinician directly during the visit, or request copies of your medical records or test reports from the administrative/medical records desk. Because the grade and number on the report are key indicators for deciding the treatment plan, it’s recommended to take a photo or record them separately for your own reference.
Q. If I choose active surveillance and the cancer grows, isn’t that dangerous?
Active surveillance assumes regular ultrasound follow-up based on a clinician-defined protocol. If meaningful growth or suspicious lymph node findings meet the predefined criteria, surgery is performed. Research trends have reported that, with appropriate patient selection and timely conversion to surgery when indicated, outcomes are not markedly different from immediate surgery.
Q. Which is better: lobectomy (partial removal) or total thyroidectomy?
This is decided by considering tumor size, location, number of lesions, and whether lymph node metastasis is present. Lobectomy has the advantage of lowering the likelihood of needing thyroid hormone medication, while total thyroidectomy can make recurrence-risk management and follow-up (including blood tests) more straightforward. Recently, there has been a tendency to aim for the minimum necessary extent when possible to support quality of life, but the decision depends on individual circumstances.
Q. When is the best time to schedule a consultation or visit?
If you can feel a neck lump, if hoarseness lasts more than two weeks, or if you have difficulty swallowing, a diagnostic evaluation is needed. Also, if a health checkup found a nodule but you did not receive a clear explanation of risk and you remain anxious, bringing your results and consulting a specialist to reassess risk can be helpful.

Thyroid disease information can be vast and confusing. To choose the right hospital and medical team, remember these three points.
First, confirm an objective risk category (K-TIRADS, Bethesda) as a number—not just a vague sense of anxiety.
Second, look for clinicians who will discuss the pros and cons of surgery versus active surveillance in a way that fits your lifestyle and values.
Third, check whether the system has a concrete long-term management plan for issues that may arise after treatment.
If you use the question list summarized today and communicate thoroughly with your medical team, it can greatly help you find the path that fits your body and situation.
Sources
- 대한갑상선학회, 갑상선 결절 및 암 진료 권고안
- 국립암센터, 국가암정보센터 갑상선암 정보
- USPSTF, Screening for Thyroid Cancer, JAMA, 2017
※ The copyright for all content on this blog belongs to medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.
Recommended reads
