
During implant surgery, visualizing hazardous structures such as nerve canals through imaging and incorporating a safety margin into the treatment plan is essential for increasing predictability. We provide clear criteria for how digital guides manage potential errors and verify accuracy through documented results.
"What if the nerve is touched during surgery, causing sensory abnormalities?"
"Does using a guide eliminate the risk of errors or side effects entirely?"
Fear regarding surgical side effects, tingling, or sensory loss is a very natural response when facing treatment. This anxiety is often heightened for procedures in areas like the posterior lower jaw, where nerve canals are located in close proximity. The thought of undergoing surgery inside the jawbone, which is not visible to the naked eye, can be a significant psychological burden.
To alleviate vague anxiety, it is more practical to review verifiable procedures rather than relying on optimistic reassurances. We have organized objective criteria regarding which imaging techniques are selected to understand bone condition and how potential errors during surgery are minimized.
1. What imaging should be verified to reduce the risk of sensory issues in mandibular implants?
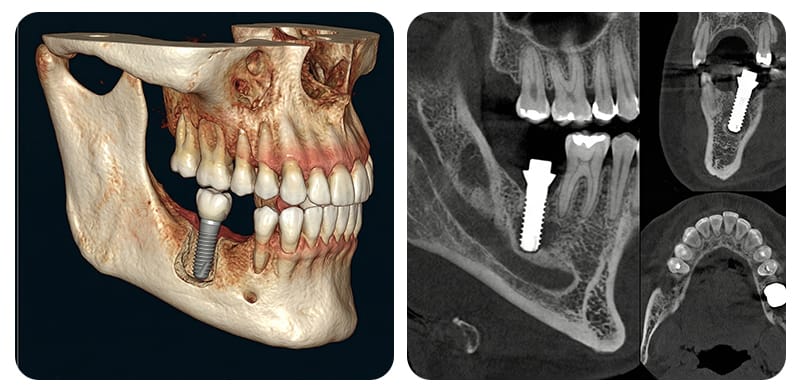
The posterior area of the lower jaw is the pathway for the inferior alveolar nerve (IAN), a critical complex of nerves and blood vessels. If an implant is placed too close to this canal, sensory abnormalities such as tingling or numbness can occur. Therefore, a diagnostic process that multi-dimensionally analyzes the bone's three-dimensional state is paramount.
According to evidence-based recommendations in Korea, a staged imaging diagnosis is standard to maintain a balance between safety and radiation exposure.
Generally, 2D imaging such as panoramas or intraoral X-rays is used first to observe the general path. CBCT (Cone Beam Computed Tomography) is selectively added when the nerve canal's location is unclear or when cross-sectional information is required. Through the secured 3D images, the path and variations of the nerve canal are analyzed to set a conservative safety margin.
While a "2mm safety margin" from the nerve canal is frequently mentioned in literature, it cannot be stated that this figure alone prevents sensory issues. This is because various indirect factors—such as the type of anesthesia, the extent of the gum incision, minute tool tolerances, and individual anatomical differences—all play a role. Therefore, we recommend clearly verifying the following criteria before treatment:
- Whether there are clear standards for adding a CBCT when the nerve location is unclear or high risk is suspected after the initial 2D evaluation.
- Whether the 3D images are meticulously interpreted to account for individual anatomical variations and the nerve's path.
- Whether a sufficiently conservative safety margin is designed to account for unexpected errors, and if its significance is clearly explained.
2. How do Korean digital guides and navigation systems check and manage errors?
Computer-aided surgery is an approach that plans the surgical path in advance through 3D simulation and reproduces it in the actual oral environment.
Implementing the planned angle and position through a physical device is called a "static guide," while tracking the current position of the tools on a real-time monitor is referred to as "dynamic navigation." While these digital tools help improve surgical precision, they do not mean that every surgical error is completely removed.
Minute deviations can accumulate during the registration stage (merging oral scan data with CT images), the process of manufacturing the guide device with a 3D printer, and when firmly fixing the device in the mouth. Mechanical gaps created by rotating drills or instability in tool manipulation due to a narrow field of view can also cause errors. Therefore, the practical standard for evaluation is not the brand of equipment, but the rigor of the management system:
- Procedures to verify that the manufactured guide device is firmly fixed and fits snugly against the teeth and gums without any gaps.
- A planning process that incorporates a generous safety margin, considering the minute vibrations or tolerances of the drill from the start.
- Clear transition criteria for immediately switching the surgical method if the actual bone shape differs from expectations during surgery.
- A system for checking the actual placement post-surgery and transparently sharing the surgical records and verification results.
3. How should expats design their visit schedule and aftercare for safety?
International patients planning treatment in Korea often feel pressured to finish all surgeries within a limited stay. However, adopting a digital guide method does not necessarily mean the number of Visits or the duration of the Stay will be reduced.
The recovery process varies depending on whether bone grafting or sinus procedures are involved, the proximity to nerve canals, and systemic health. Designing a plan that includes Aftercare after returning home is the key to long-term safety.
It is advisable to establish conservative schedules and response systems in advance based on individual health and surgical scope:
- Case A: If surgery is performed near the posterior mandibular nerve canal, it is safer to include a stay duration that allows for monitoring for any sensory abnormalities like tingling or pain before returning home.
- Case B: If additional sinus-related procedures are involved, bleeding and swelling must be closely monitored; thus, the flight schedule should be conservatively adjusted according to the recovery progress.
- Case C: For those taking medications that affect bone metabolism or those in high-risk groups for systemic diseases, it is helpful to secure English prescriptions and records to ensure medical status can be tracked and monitored.
- Case D: If conscious sedation is used due to severe dental anxiety, verify a monitoring environment where spontaneous breathing and responses are maintained, and plan a trip home with a companion after sufficient rest post-sedation.
To reduce concerns about sensory abnormalities, please check these three core criteria:
First, ensure that 2D and CBCT imaging are used staged to meticulously analyze the nerve location and maintain a conservative safety margin.
Second, verify if there are clear criteria for transitioning the surgical plan during the procedure, acknowledging the possibility of guide device errors.
Third, for those living abroad, check if the clinic systematically provides medical records and imaging data so that seamless aftercare is possible after your return.
No digital equipment can ensure zero nerve damage or side effects. Rather than relying on a specific technology or device name, we sincerely support you in proceeding with treatment more comfortably by checking whether thorough diagnostic and verification procedures are in place.
Sources
- Lee et al., Development of Recommendations for Dental Implant Imaging Diagnosis, 2020
- Bae & Lee, Systematic Review of Clinical Precautions for Computer-Guided Surgery, 2021
- Meta-analysis related to the accuracy of computer-aided surgery (static/dynamic)
※ The copyright for all content on this blog belongs to medihi. Unauthorized copying, distribution, or derivative use is strictly prohibited, and violations may result in legal action without prior notice.
Recommended reads
